

Correlation between genomic index lesions and mpMRI and 68Ga-PSMA-PET/CT imaging features in primary prostate cancer
- PMID: 30420756
- PMCID: PMC6232089
- DOI: 10.1038/s41598-018-35058-3
Correlation between genomic index lesions and mpMRI and 68Ga-PSMA-PET/CT imaging features in primary prostate cancer
Abstract
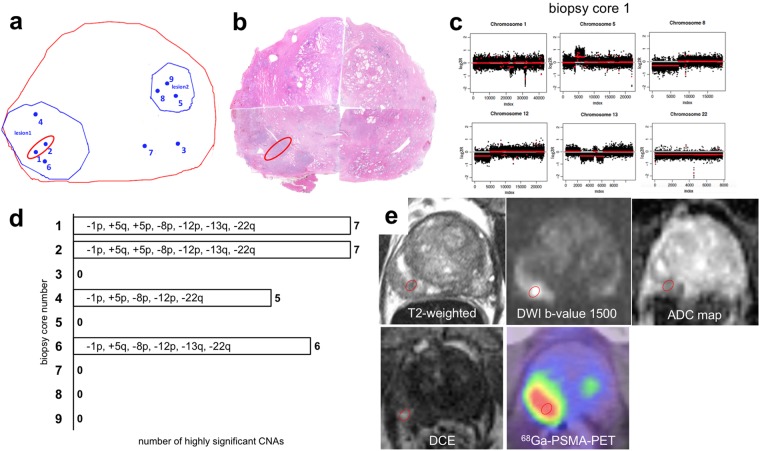
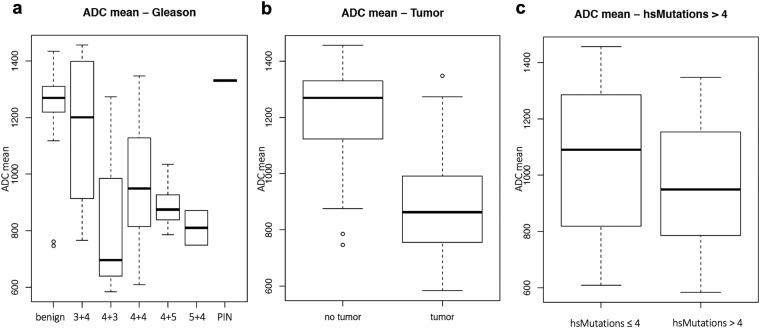
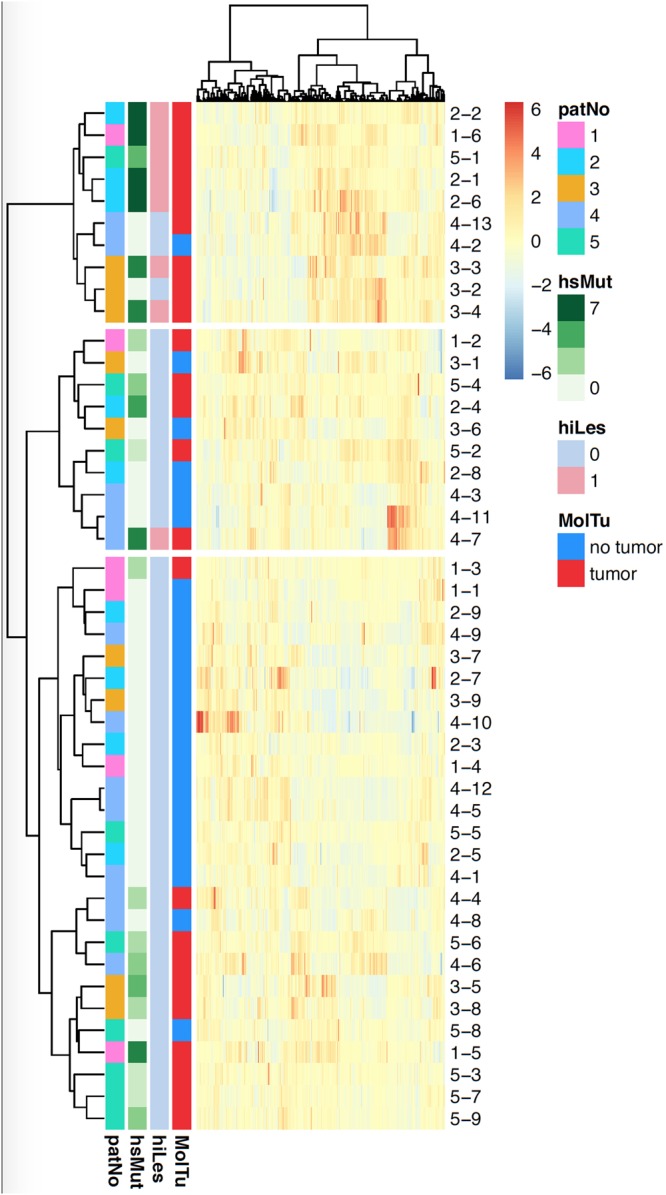
Magnetic resonance imaging (MRI) and prostate specific membrane antigen (PSMA)- positron emission tomography (PET)/computed tomography (CT)-imaging of prostate cancer (PCa) are emerging techniques to assess the presence of significant disease and tumor progression. It is not known, however, whether and to what extent lesions detected by these imaging techniques correlate with genomic features of PCa. The aim of this study was therefore to define a genomic index lesion based on chromosomal copy number alterations (CNAs) as marker for tumor aggressiveness in prostate biopsies in direct correlation to multiparametric (mp) MRI and 68Ga-PSMA-PET/CT imaging features. CNA profiles of 46 biopsies from five consecutive patients with clinically high-risk PCa were obtained from radiologically suspicious and unsuspicious areas. All patients underwent mpMRI, MRI/TRUS-fusion biopsy, 68Ga-PSMA-PET/CT and a radical prostatectomy. CNAs were directly correlated to imaging features and radiogenomic analyses were performed. Highly significant CNAs (≥10 Mbp) were found in 22 of 46 biopsies. Chromosome 8p, 13q and 5q losses were the most common findings. There was an strong correspondence between the radiologic and the genomic index lesions. The radiogenomic analyses suggest the feasibility of developing radiologic signatures that can distinguish between genomically more or less aggressive lesions. In conclusion, imaging features of mpMRI and 68Ga-PSMA-PET/CT can guide to the genomically most aggressive lesion of a PCa. Radiogenomics may help to better differentiate between indolent and aggressive PCa in the future.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
