

Neoadjuvant Dose-dense Gemcitabine and Cisplatin in Muscle-invasive Bladder Cancer: Results of a Phase 2 Trial
- PMID: 30420974
- PMCID: PMC6226048
- DOI: 10.1016/j.euo.2018.02.007
Neoadjuvant Dose-dense Gemcitabine and Cisplatin in Muscle-invasive Bladder Cancer: Results of a Phase 2 Trial
Abstract
Background: Accelerated (also termed dose-dense, DD) chemotherapy regimens such as accelerated methotrexate, vinblastine, doxorubicin, and cisplatin have shown better efficacy and tolerability in the metastatic setting, and shortened the time to surgery in the neoadjuvant setting compared to standard-schedule regimens. We hypothesized that a DD schedule of gemcitabine and cisplatin (GC) would shorten the time to surgery and yield similar pathologic complete response rates (pT0) in patients with muscle-invasive bladder cancer (MIBC) compared with historical controls with standard GC.
Objective: To determine the safety and efficacy of neoadjuvant DDGC in MIBC.
Design setting and participants: Patients with cT2-4a, N0-1, M0 MIBC were eligible and received three 14-d cycles of DDGC with pegfilgrastim support followed by radical cystectomy with lymph node dissection. The primary end point was the pT0 rate. Molecular subtypes were assigned and correlated with survival.
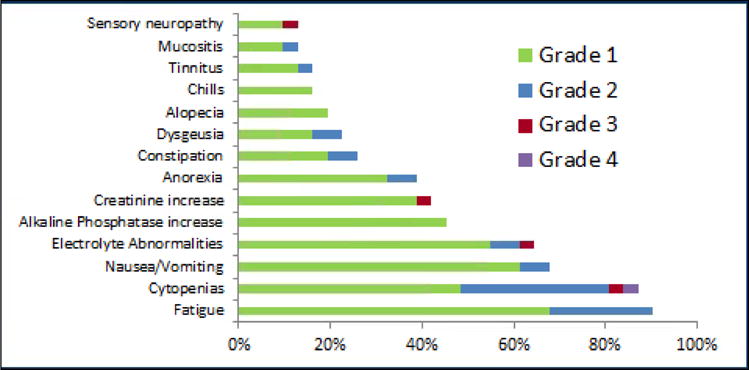
Results and limitations: Thirty-one patients were evaluable for toxicity and response, of whom 58% had baseline clinical stage >T2N0M0; the median age was 69 yr. Ten patients (32%, 95% confidence interval [CI] 16-49%) achieved ypT0N0 status at cystectomy. Another four patients (13%, 95% CI 1-25%) were downstaged to non-muscle-invasive (<pT2N0) disease. Most patients (54.8%) experienced only grade 1-2 treatment-related toxicities. However, seven patients (23%) had clinically significant vascular events, leading to early closure of the study. Thirty patients (94%) underwent cystectomy. The median time from the start of chemotherapy to cystectomy was 9.3 wk. There was no correlation between molecular subtypes and survival.
Conclusions: DDGC yielded a similar pT0 rate to that noted retrospectively with standard GC. Vascular events precluded, delayed, or increased the risk of surgery for 23% of patients, resulting in early closure of the study. Additional prospective studies with embedded biomarker correlatives of GC in the neoadjuvant setting are critical to accurately define both the activity and toxicity of this combination in MIBC.
Patient summary: Neoadjuvant chemotherapy before cystectomy is the standard of care for muscle-invasive bladder cancer (MIBC). This prospective phase 2 study tested a dose-dense schedule of gemcitabine and cisplatin in MIBC. The study was closed early because of a higher than expected rate of vascular events. These data suggest that caution is required in using this regimen, particularly when there is better prospective evidence for the safety and efficacy of alternative regimens such as dose-dense or accelerated methotrexate, vinblastine, doxorubicin, and cisplatin.
Conflict of interest statement
Financial disclosures: Elizabeth R. Plimack certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: None.
Figures


References
-
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349:859–66. - PubMed
-
- Plimack ER, Hoffman-Censits JH, Viterbo R, et al. Accelerated methotrexate, vinblastine, doxorubicin, and cisplatin is safe, effective, and efficient neoadjuvant treatment for muscle-invasive bladder cancer: results of a multicenter phase II study with molecular correlates of response and toxicity. J Clin Oncol. 2014;32:1895–901. - PMC - PubMed
-
- von der Maase H, Hansen SW, Roberts JT, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol. 2000;18:3068–77. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous