

Swallowing MRI-a reliable method for the evaluation of the postoperative gastroesophageal situs after Nissen fundoplication
- PMID: 30421012
- PMCID: PMC6610269
- DOI: 10.1007/s00330-018-5779-2
Swallowing MRI-a reliable method for the evaluation of the postoperative gastroesophageal situs after Nissen fundoplication
Abstract
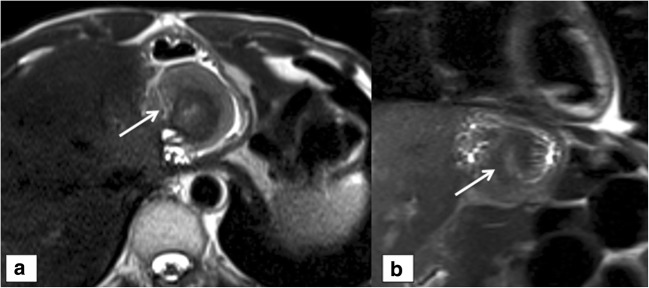
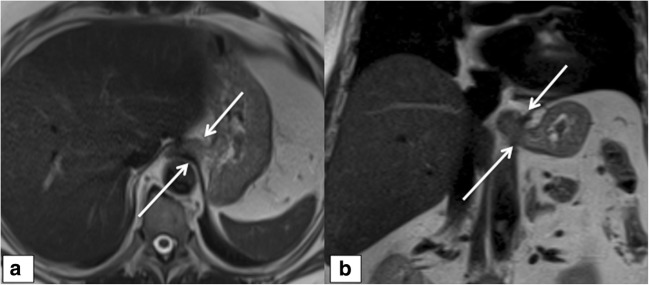
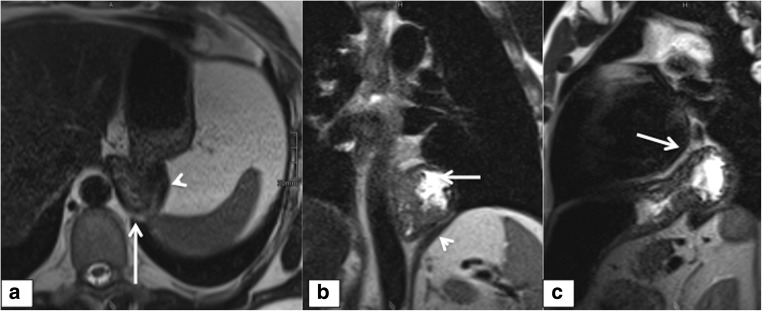
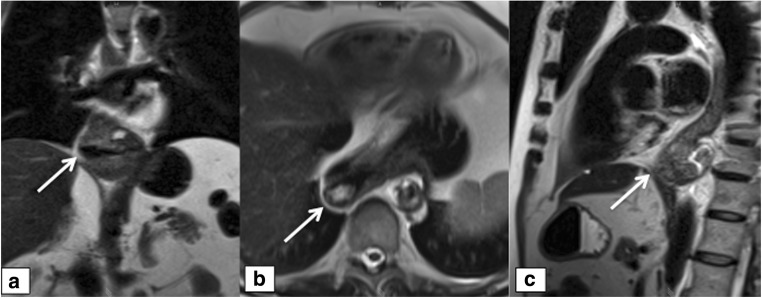
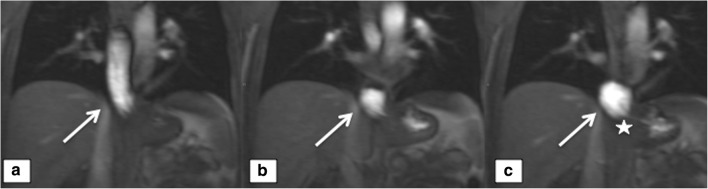
Purpose: To evaluate the diagnostic performance of swallowing MRI of the gastroesophageal junction (GEJ) in the postoperative care of patients after laparoscopic antireflux surgery (LARS) MATERIAL AND METHODS: In this institutional review board-approved prospective study, 79 symptomatic patients (mean age, 52.3 years; range, 26-80 years) were evaluated after laparoscopic Nissen fundoplication. MRI findings were correlated with revision surgery, endoscopy, and high-resolution manometry (HRM) as standard of reference. MRI was performed on a 3.0-T unit using T2-weighted half-Fourier acquisition single-shot turbo spin echo (HASTE) sequences for anatomical assessment of the GEJ followed by dynamic MR swallowing (fast low-angle shot sequences). Four independent readers (two radiologists, two surgeons) rated 83 MR scans according to defined criteria, such as wrap disruption, slipping, recurrent hiatal hernia, and esophageal motility disorder.
Results: Wrap disruption was correctly diagnosed concordantly with the standard of reference in 87.8%, slipping in 81.5%, and recurrent hiatal hernia in 84.9% of the cases. For esophageal motility disorder, MRI interpretation was consistent with manometry in 66.2% of the subjects. Interobserver analysis showed substantial agreement for recurrent hiatal hernia (k = 0.703), moderate agreement for wrap disruption (k = 0.585), and fair agreement for motility disorder and slipping (k = 0.234 and k = 0.200, respectively).
Conclusion: MR swallowing readily depicts the major failure mechanisms of LARS and has good reliability even in non-experienced readers.
Key points: • MR swallowing accurately readily depicts the major failure mechanisms of laparoscopic antireflux surgery and has good reliability even in non-experienced readers. • It should be included in the preoperative workup for revision surgery after fundoplication. • It will be of great benefit to surgeons in considering and planning a reoperation.
Keywords: Fundoplication; GERD; Magnetic resonance imaging.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
References
-
- Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, Lombard R. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc. 1991;1:138. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
