

Alcohol Intake and Weight Loss During Intensive Lifestyle Intervention for Adults with Overweight or Obesity and Diabetes
- PMID: 30421851
- PMCID: PMC6309276
- DOI: 10.1002/oby.22316
Alcohol Intake and Weight Loss During Intensive Lifestyle Intervention for Adults with Overweight or Obesity and Diabetes
Erratum in
-
Erratum: Alcohol Intake and Weight Loss During Intensive Lifestyle Intervention for Adults with Overweight or Obesity and Diabetes.Obesity (Silver Spring). 2019 Apr;27(4):678. doi: 10.1002/oby.22442. Epub 2019 Feb 27. Obesity (Silver Spring). 2019. PMID: 30900407 No abstract available.
Abstract
Objective: This study aimed to assess whether alcohol consumption decreases during an intensive lifestyle intervention (ILI) and whether alcohol consumption is associated with weight loss among participants with overweight or obesity and type 2 diabetes.
Methods: Participants (n = 4,901) were from the Action for Health in Diabetes (Look AHEAD) study, a randomized controlled trial that compared an ILI with a diabetes support and education (DSE) control. Mixed-effects models were used to estimate the effect of the ILI on alcohol consumption and the influence of alcohol consumption on weight loss at year 4.
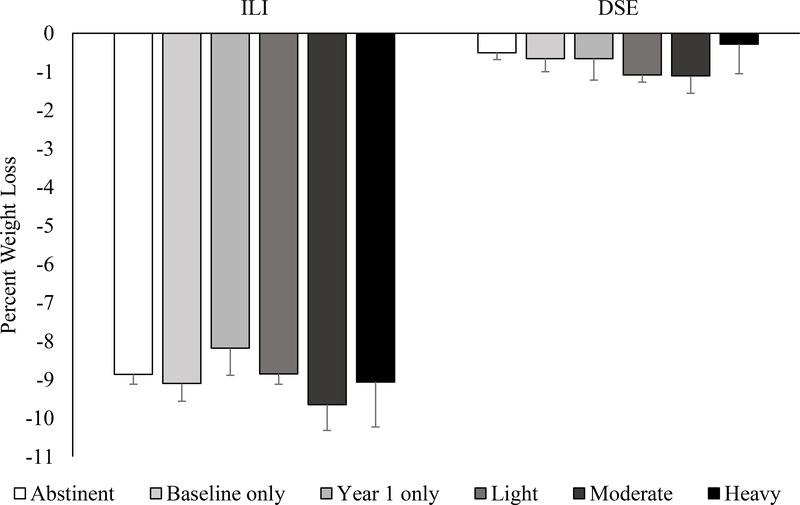
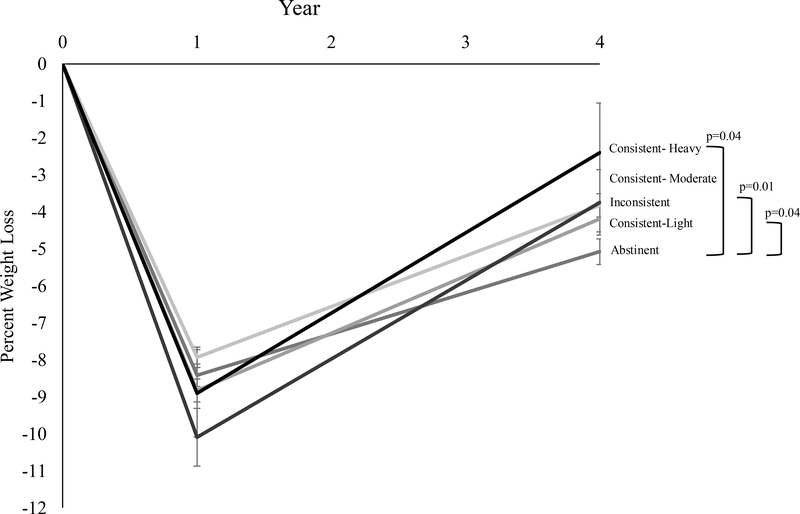
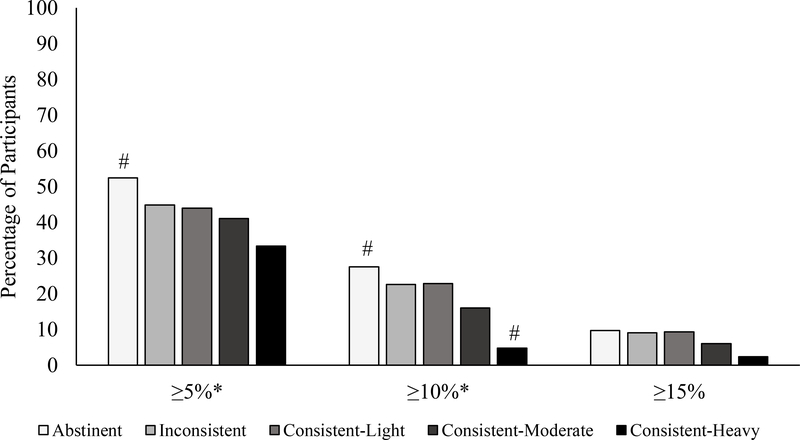
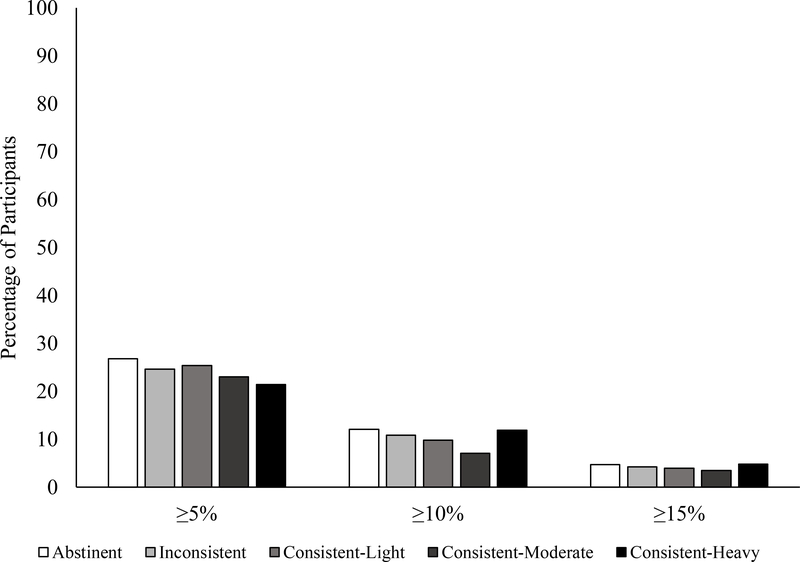
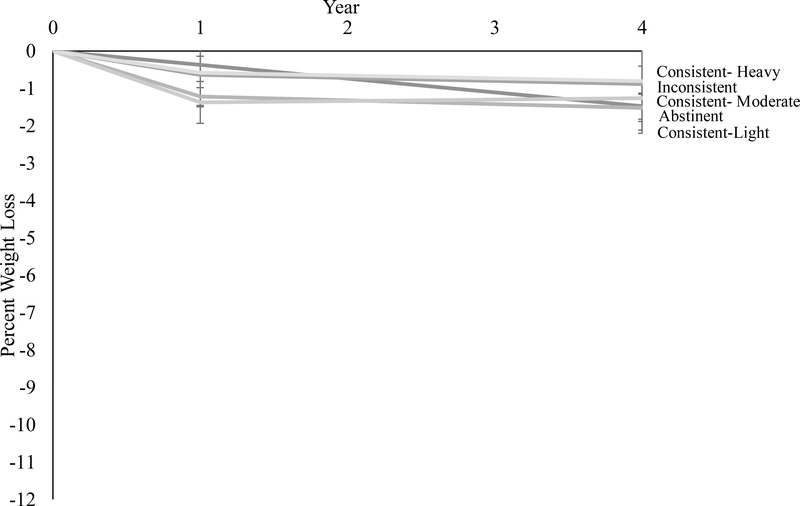
Results: ILI and DSE participants did not differ in changes in alcohol consumption. Alcohol intake was not associated with weight loss at year 1 of the ILI. ILI participants who abstained from alcohol lost 5.1% ± 0.3% of initial weight at year 4 compared with a significantly (P = 0.04) smaller 2.4% ± 1.3% for consistent heavy drinkers. ILI participants who abstained from alcohol consumption over the 4 years lost 1.6% ± 0.5% more weight relative to individuals who drank alcohol at any time during the intervention (P = 0.003). DSE participants did not differ in weight loss by alcohol consumption.
Conclusions: Heavy alcohol drinkers are at risk for suboptimal long-term weight loss. Decreasing alcohol consumption may improve weight management among individuals with diabetes.
Trial registration: ClinicalTrials.gov NCT00017953.
© 2018 The Obesity Society.
Figures
References
-
- Center for Behavioral Health Statistics and Quality. Behavioral health trends in the United States: results from the 2014 National Survey on Drug Use and Health. Rockville, MD, USA: 2015. HHS Publication No. SMA 15–4927, NSDUH Series H-50.
-
- Grant BF, Chou SP, Saha TD, et al. Prevalence of 12-month alcohol use, high-risk drinking, and DSM-IV alcohol use disorder in the United States, 2001–2002 to 2012–2013: results from the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry. 2017;74(9):911–923. - PMC - PubMed
-
- Li X-H, Yu F-f, Zhou Y-H, He J. Association between alcohol consumption and the risk of incident type 2 diabetes: a systematic review and dose-response meta-analysis. The American Journal of Clinical Nutrition. 2016;103(3):818–829. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U01 DK057151/DK/NIDDK NIH HHS/United States
- U01 DK057154/DK/NIDDK NIH HHS/United States
- U01 DK057171/DK/NIDDK NIH HHS/United States
- U01 DK057182/DK/NIDDK NIH HHS/United States
- U01 DK057136/DK/NIDDK NIH HHS/United States
- U01 DK057002/DK/NIDDK NIH HHS/United States
- U01 DK057177/DK/NIDDK NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- U01 DK057078/DK/NIDDK NIH HHS/United States
- U01 DK048514/DK/NIDDK NIH HHS/United States
- U01 DK057149/DK/NIDDK NIH HHS/United States
- K23 NR017209/NR/NINR NIH HHS/United States
- P30 DK048520/DK/NIDDK NIH HHS/United States
- U01 DK057135/DK/NIDDK NIH HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- DH_/Department of Health/United Kingdom
- P30 DK046204/DK/NIDDK NIH HHS/United States
- M01 RR002719/RR/NCRR NIH HHS/United States
- M01 RR000056/RR/NCRR NIH HHS/United States
- U01 DK057219/DK/NIDDK NIH HHS/United States
- K23 DK116935/DK/NIDDK NIH HHS/United States
- U01 DK056992/DK/NIDDK NIH HHS/United States
- U01 DK057131/DK/NIDDK NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- U01 DK056990/DK/NIDDK NIH HHS/United States
- U01 DK057178/DK/NIDDK NIH HHS/United States
- M01RR0021140/GF/NIH HHS/United States
- U01 DK057008/DK/NIDDK NIH HHS/United States
- M01 RR001346/RR/NCRR NIH HHS/United States
- CC/CDC HHS/United States
