

Effect of a Pharmacist-Led Educational Intervention on Inappropriate Medication Prescriptions in Older Adults: The D-PRESCRIBE Randomized Clinical Trial
- PMID: 30422193
- PMCID: PMC6248132
- DOI: 10.1001/jama.2018.16131
Effect of a Pharmacist-Led Educational Intervention on Inappropriate Medication Prescriptions in Older Adults: The D-PRESCRIBE Randomized Clinical Trial
Abstract
Importance: High rates of inappropriate prescribing persist among older adults in many outpatient settings, increasing the risk of adverse drug events and drug-related hospitalizations.
Objective: To compare the effectiveness of a consumer-targeted, pharmacist-led educational intervention vs usual care on discontinuation of inappropriate medication among community-dwelling older adults.
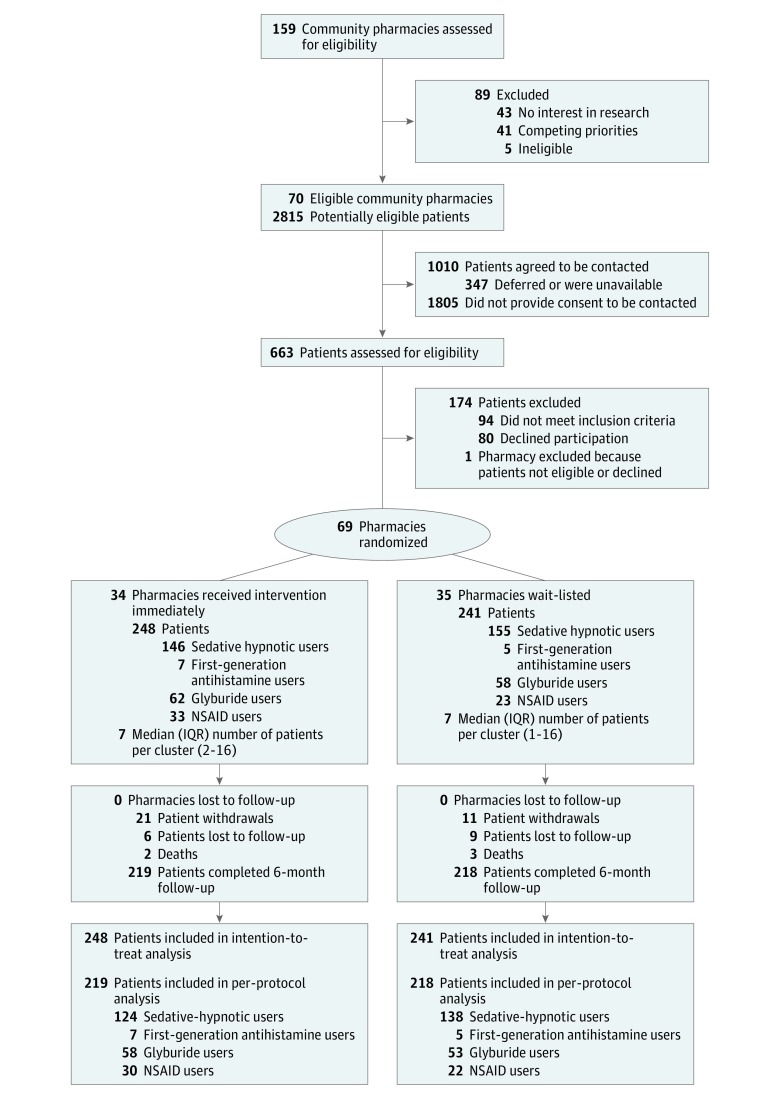
Design, setting, and participants: A cluster randomized trial (D-PRESCRIBE [Developing Pharmacist-Led Research to Educate and Sensitize Community Residents to the Inappropriate Prescriptions Burden in the Elderly]) that recruited community pharmacies in Quebec, Canada, from February 2014 to September 2017, with follow-up until February 2018, and randomly allocated them to intervention or control groups. Patients included were adults aged 65 years and older who were prescribed 1 of 4 Beers Criteria medications (sedative-hypnotics, first-generation antihistamines, glyburide, or nonsteroidal anti-inflammatory drugs), recruited from 69 community pharmacies. Patients were screened and enrolled before randomization.
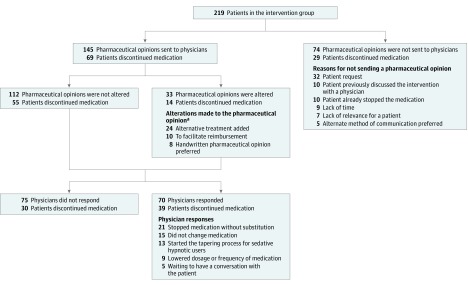
Interventions: Pharmacists in the intervention group were encouraged to send patients an educational deprescribing brochure in parallel to sending their physicians an evidence-based pharmaceutical opinion to recommend deprescribing. The pharmacists in the control group provided usual care. Randomization occurred at the pharmacy level, with 34 pharmacies randomized to the intervention group (248 patients) and 35 to the control group (241 patients). Patients, physicians, pharmacists, and evaluators were blinded to outcome assessment.
Main outcomes and measures: Discontinuation of prescriptions for inappropriate medication at 6 months, ascertained by pharmacy medication renewal profiles.
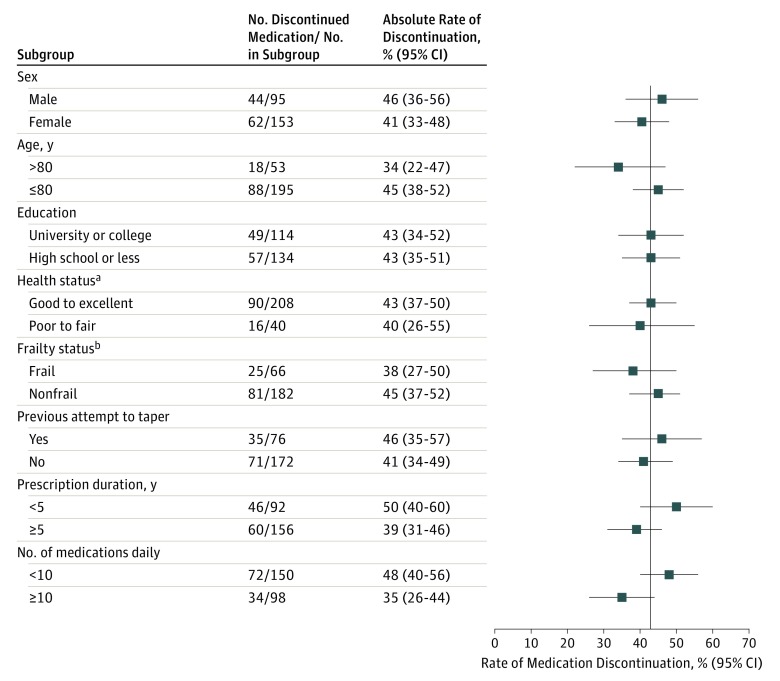
Results: Among 489 patients (mean age, 75 years; 66% women), 437 (89%) completed the trial (219 [88%] in the intervention group vs 218 [91%] in the control group). At 6 months, 106 of 248 patients (43%) in the intervention group no longer filled prescriptions for inappropriate medication compared with 29 of 241 (12%) in the control group (risk difference, 31% [95% CI, 23% to 38%]). In the intervention vs control group, discontinuation of inappropriate medication occurred among 63 of 146 sedative-hypnotic drug users (43.2%) vs 14 of 155 (9.0%), respectively (risk difference, 34% [95% CI, 25% to 43%]); 19 of 62 glyburide users (30.6%) vs 8 of 58 (13.8%), respectively (risk difference, 17% [95% CI, 2% to 31%]); and 19 of 33 nonsteroidal anti-inflammatory drug users (57.6%) vs 5 of 23 (21.7%), respectively (risk difference, 35% [95% CI, 10% to 55%]) (P for interaction = .09). Analysis of the antihistamine drug class was not possible because of the small sample size (n = 12). No adverse events requiring hospitalization were reported, although 29 of 77 patients (38%) who attempted to taper sedative-hypnotics reported withdrawal symptoms.
Conclusions and relevance: Among older adults in Quebec, a pharmacist-led educational intervention compared with usual care resulted in greater discontinuation of prescriptions for inappropriate medication after 6 months. The generalizability of these findings to other settings requires further research.
Trial registration: ClinicalTrials.gov Identifier: NCT02053194.
Conflict of interest statement
Figures
Comment in
-
Overcoming Inertia to Improve Medication Use and Deprescribing.JAMA. 2018 Nov 13;320(18):1867-1869. doi: 10.1001/jama.2018.16473. JAMA. 2018. PMID: 30422182 Free PMC article. No abstract available.
-
Pharmacist-Led Education to Discontinue Inappropriate Prescribing.JAMA. 2019 Apr 2;321(13):1313-1314. doi: 10.1001/jama.2019.0302. JAMA. 2019. PMID: 30938791 No abstract available.
References
-
- Canadian Institute for Health Information Drug Use Among Seniors in Canada, 2016. Ottawa, ON: Canadian Institute for Health Information; 2018. https://www.cihi.ca/sites/default/files/document/drug-use-among-seniors-.... Accessed September 14, 2018.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
