

Effect of a Lay Counselor Intervention on Prevention of Major Depression in Older Adults Living in Low- and Middle-Income Countries: A Randomized Clinical Trial
- PMID: 30422259
- PMCID: PMC6583466
- DOI: 10.1001/jamapsychiatry.2018.3048
Effect of a Lay Counselor Intervention on Prevention of Major Depression in Older Adults Living in Low- and Middle-Income Countries: A Randomized Clinical Trial
Abstract
Importance: Preventing depression in older adults living in low- and middle-income countries is important because of the scarcity of treatment resources and the risk of disability, suicide, and dementia.
Objective: To assess whether an intervention for depression prevention provided by lay counselors is effective in older adults from low- and middle-income countries.
Design, setting, and participants: This parallel-group randomized clinical trial with masked outcome assessment was performed in 181 older adults (≥60 years) with subsyndromal depressive symptoms at rural and urban primary care clinics in Goa, India. The first participant entered the trial on March 31, 2015, and the last exited on June 2, 2017. Data analysis used the intention-to-treat approach.
Interventions: Lay counselors provided problem-solving therapy, brief behavioral treatment for insomnia, education in self-care of common medical disorders such as diabetes, and assistance in accessing medical and social programs.
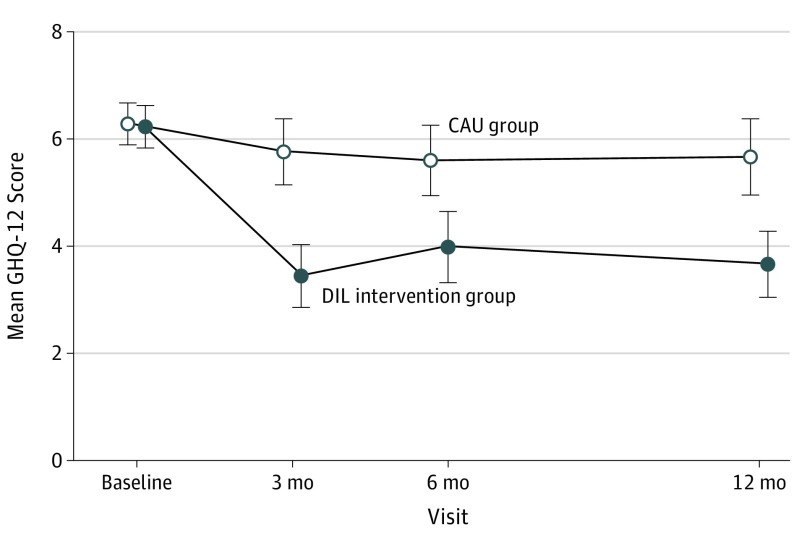
Main outcomes and measures: The main outcome was incidence of major depressive episodes. The study also assessed symptom change during 12 months (12-item General Health Questionnaire [GHQ-12]; score range of 0 to 12, with higher scores indicating greater symptoms of depression and anxiety), functional status (World Health Organization Disability Assessment Schedule 2.0; score range of 12 to 60, with higher scores indicating greater disability), cognition (Hindi Mini-Mental State Examination; score range of 0 to 30, with higher scores indicating better cognitive functioning), blood pressure, and body mass index to provide further clinical context.
Results: The study enrolled 181 participants (mean [SD] age, 69.6 [7.2] years; 114 [63.0%] female): 91 to the intervention arm (depression in later life [DIL] intervention) and 90 to care as usual (CAU). Incident episodes of major depression were lower in the DIL intervention than in the CAU group (4.40% vs 14.44%; log-rank P = .04; number needed to treat, 9.95; 95% CI, 5.12-182.43). The 12-month Kaplan-Meier estimates of percentage of depression-free participants were 95.1% (95% CI, 90.5%-99.9%) in the DIL group vs 87.4% (95% CI, 80.4%-95.1%) in the CAU group. The incidence of depressive symptoms (GHQ-12) was also less (12-month mean difference, -1.18; 95% CI, -2.03 to -0.31; group × time interaction P < .001). There were no changes in measures of disability or cognition. The DIL intervention was associated with a significantly greater lowering of systolic blood pressure (12-month mean difference, -6.98; 95% CI, -11.96 to -2.01; group × time interaction P < .001) and change in body mass index (12-month mean difference, 0.23; 95% CI, -0.97 to 1.43; P = .04).
Conclusions and relevance: The DIL intervention is effective for preventing episodes of major depression in older persons with subsyndromal symptoms. If replicated, the DIL intervention may be effective in older adults living in low- and middle-income countries.
Trial registration: ClinicalTrials.gov Identifier: NCT02145429.
Conflict of interest statement
Figures


Comment in
-
Preventing Late-Life Depression Through Task Sharing: Scope of Translating Evidence to Practice in Resource-Scarce Settings.JAMA Psychiatry. 2019 Jan 1;76(1):7-8. doi: 10.1001/jamapsychiatry.2018.2898. JAMA Psychiatry. 2019. PMID: 30419119 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
