

Tumor-derived Autoantibodies Identify Malignant Pulmonary Nodules
- PMID: 30422669
- PMCID: PMC6519849
- DOI: 10.1164/rccm.201804-0628OC
Tumor-derived Autoantibodies Identify Malignant Pulmonary Nodules
Abstract
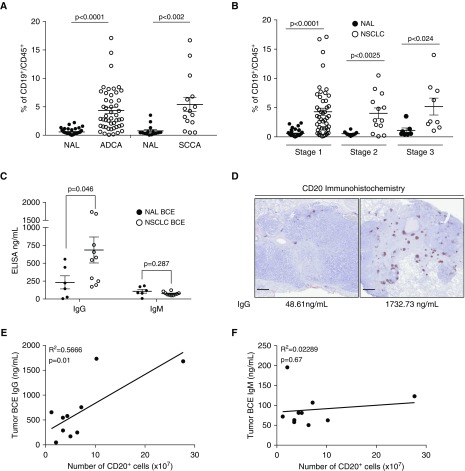
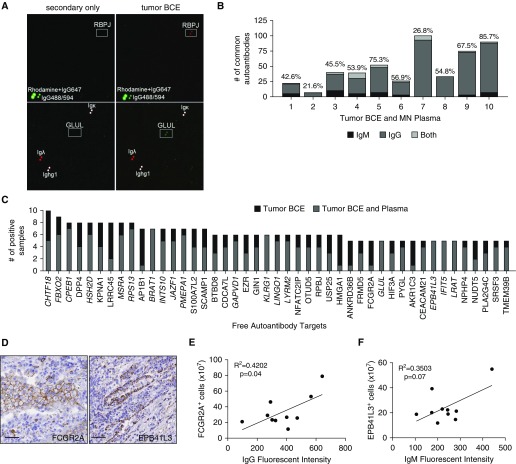
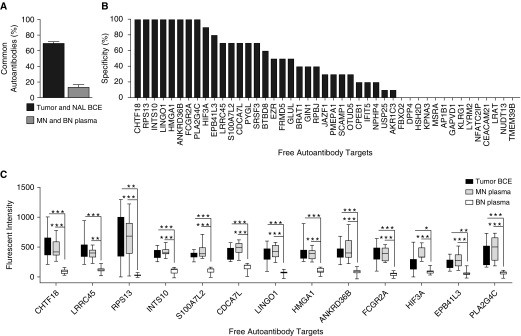
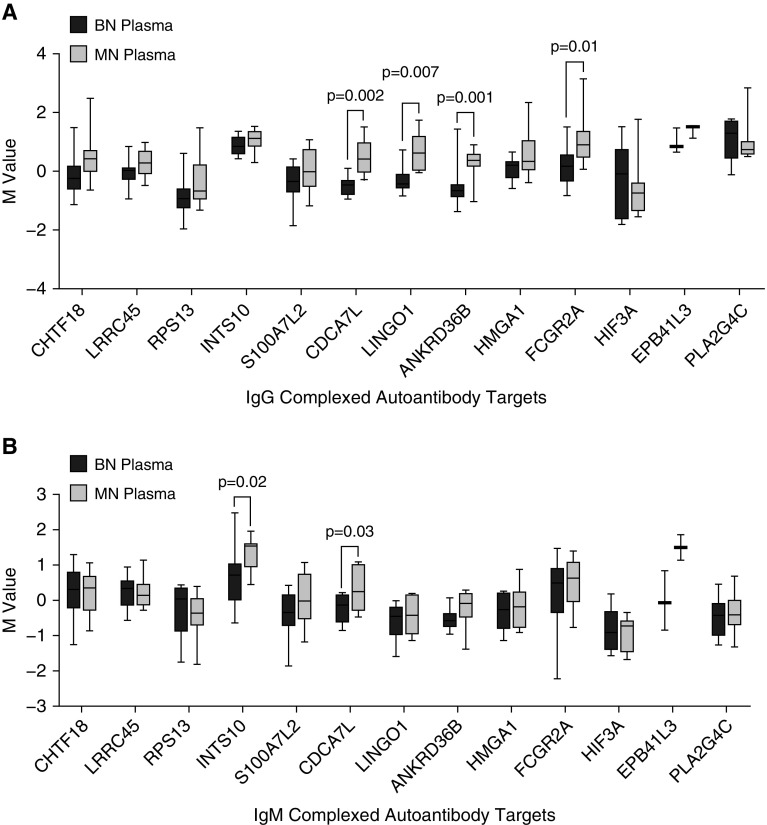
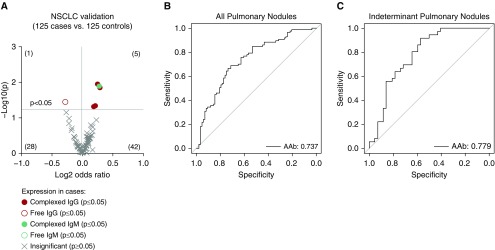
Rationale: Screening for non-small cell lung cancer is associated with earlier diagnosis and reduced mortality but also increased harm caused by invasive follow-up of benign pulmonary nodules. Lung tumorigenesis activates the immune system, components of which could serve as tumor-specific biomarkers. Objectives: To profile tumor-derived autoantibodies as peripheral biomarkers of malignant pulmonary nodules. Methods: High-density protein arrays were used to define the specificity of autoantibodies isolated from B cells of 10 resected lung tumors. These tumor-derived autoantibodies were also examined as free or complexed to antigen in the plasma of the same 10 patients and matched benign nodule control subjects. Promising autoantibodies were further analyzed in an independent cohort of 250 nodule-positive patients. Measurements and Main Results: Thirteen tumor B-cell-derived autoantibodies isolated ex vivo showed greater than or equal to 50% sensitivity and greater than or equal to 70% specificity for lung cancer. In plasma, 11 of 13 autoantibodies were present both complexed to and free from antigen. In the larger validation cohort, 5 of 13 tumor-derived autoantibodies remained significantly elevated in cancers. A combination of four of these autoantibodies could detect malignant nodules with an area under the curve of 0.74 and had an area under the curve of 0.78 in a subcohort of indeterminate (8-20 mm in the longest diameter) pulmonary nodules. Conclusions: Our novel pipeline identifies tumor-derived autoantibodies that could effectively serve as blood biomarkers for malignant pulmonary nodule diagnosis. This approach has future implications for both a cost-effective and noninvasive approach to determine nodule malignancy for widespread low-dose computed tomography screening.
Keywords: B cells; computed tomography imaging; early detection; indeterminate pulmonary nodules; lung cancer.
Figures
Comment in
-
Harnessing Immune Response to Malignant Lung Nodules. Promise and Challenges.Am J Respir Crit Care Med. 2019 May 15;199(10):1184-1186. doi: 10.1164/rccm.201811-2188ED. Am J Respir Crit Care Med. 2019. PMID: 30562043 Free PMC article. No abstract available.
References
-
- Humphrey L, Deffebach M, Pappas M, Baumann C, Artis K, Mitchell JP, et al. Screening for lung cancer: systematic review to update the US Preventive Services Task Force recommendation; US Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews. Rockville, MD: Agency for Healthcare Research and Quality; 2013. - PubMed
-
- Smith RA, Andrews KS, Brooks D, Fedewa SA, Manassaram-Baptiste D, Saslow D, et al. Cancer screening in the United States, 2017: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2017;67:100–121. - PubMed
-
- Kinsinger LS, Anderson C, Kim J, Larson M, Chan SH, King HA, et al. Implementation of lung cancer screening in the Veterans Health Administration. JAMA Intern Med. 2017;177:399–406. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
