

Primary and Repeated Respiratory Viral Infections Among Infants in Rural Nepal
- PMID: 30423150
- PMCID: PMC7317152
- DOI: 10.1093/jpids/piy107
Primary and Repeated Respiratory Viral Infections Among Infants in Rural Nepal
Abstract
Background: Respiratory viruses cause significant morbidity and death in infants; 99% of such deaths occur in resource-limited settings. Risk factors for initial and repeated respiratory viral infections in young infants in resource-limited settings have not been well described.
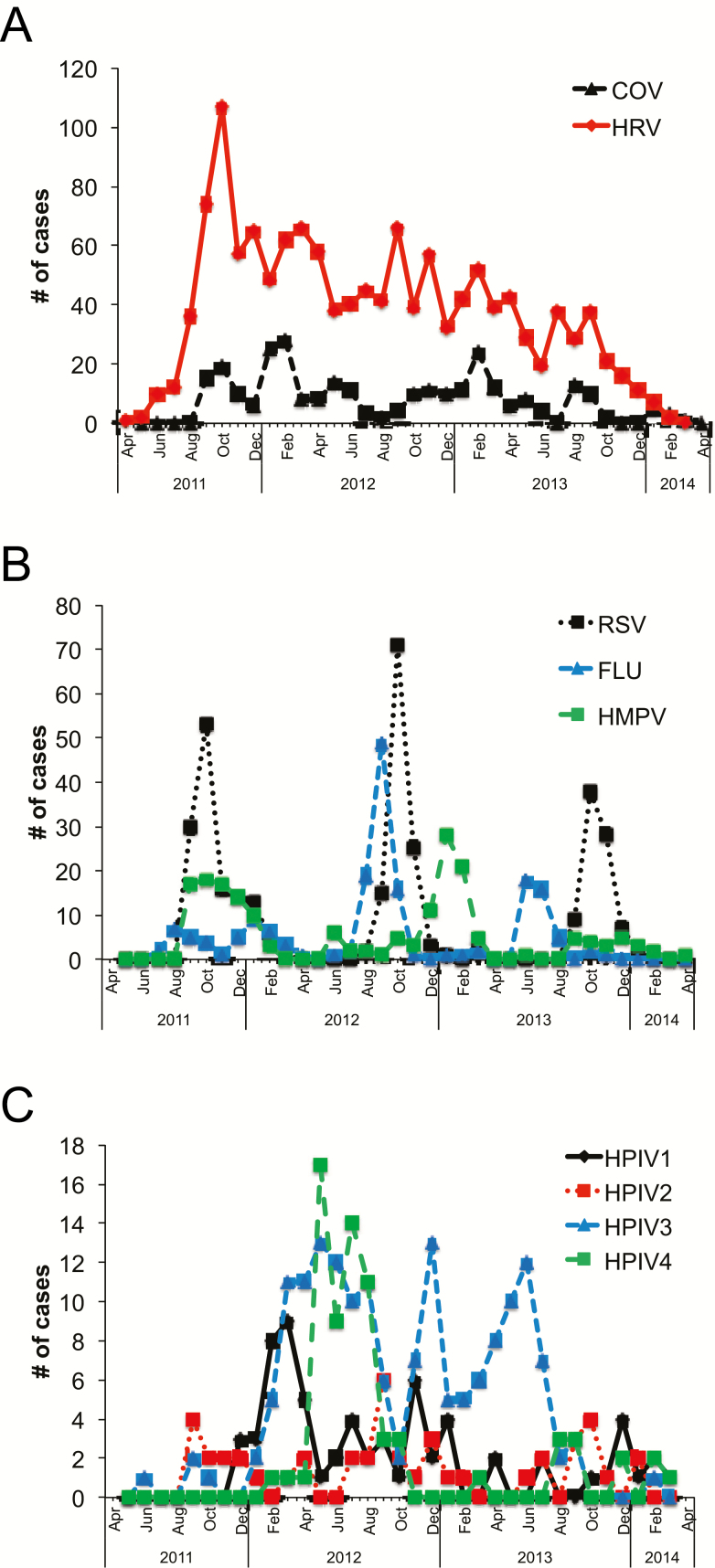
Methods: From 2011 to 2014, a birth cohort of infants in rural Nepal was enrolled and followed with weekly household-based active surveillance for respiratory symptoms until 6 months of age. Respiratory illness was defined as having any of the following: fever, cough, wheeze, difficulty breathing, and/or a draining ear. We tested nasal swabs of infants with respiratory illness for multiple respiratory viruses by using a reverse transcription polymerase chain reaction assay. The risk of primary and repeated infections with the same virus was evaluated using Poisson regression.
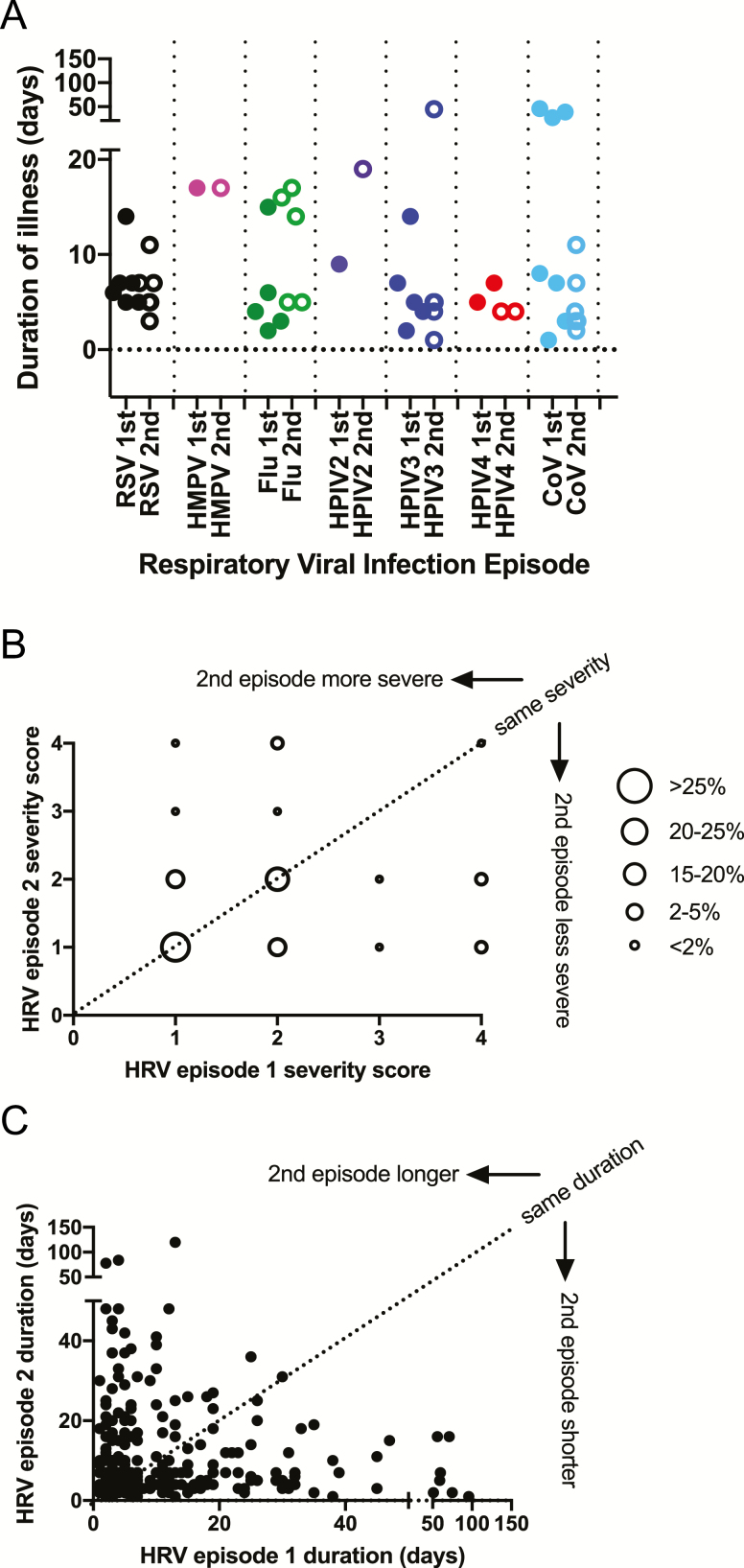
Results: Of 3528 infants, 1726 (49%) had a primary infection, and 419 (12%) had a repeated infection. The incidences of respiratory viral infection in infants were 1816 per 1000 person-years for primary infections and 1204 per 1000 person-years for repeated infection with the same virus. Exposure to other children and male sex were each associated with an increased risk for primary infection (risk ratios, 1.13 [95% confidence interval (CI), 1.06-1.20] and 1.14 [95% CI, 1.02-1.27], respectively), whereas higher maternal education was associated with a decreased risk for both primary and repeated infections (risk ratio, 0.96 [95% CI, 0.95-0.98]). The incidence of subsequent infection did not change when previous infection with the same or another respiratory virus occurred. Illness duration and severity were not significantly different in the infants between the first and second episodes for any respiratory virus tested.
Conclusions: In infants in rural Nepal, repeated respiratory virus infections were frequent, and we found no decrease in illness severity with repeated infections and no evidence of replacement with another virus. Vaccine strategies and public health interventions that provide durable protection in the first 6 months of life could decrease the burden of repeated infections by multiple respiratory viruses, particularly in low-resource countries.
Keywords: RSV; coronavirus; infants; influenza virus; parainfluenza virus; respiratory viruses; rhinovirus.
© The Author(s) 2018. Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Liu L, Mathers C, Oza S, et al. . MCEE-WHO Methods and Data Sources for Child Causes of Death 2000–2015. Geneva, Switzerland: World Health Organization; 2016; 1:20.
-
- Hall CB. Respiratory syncytial virus and parainfluenza virus. N Engl J Med 2001; 344:1917–28. - PubMed
-
- Glezen WP, Taber LH, Frank AL, Kasel JA. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child 1986; 140:543–6. - PubMed
-
- Glezen WP, Frank AL, Taber LH, Kasel JA. Parainfluenza virus type 3: seasonality and risk of infection and reinfection in young children. J Infect Dis 1984; 150:851–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
