

In Older Patients Treated for Dizziness and Vertigo in Multimodal Rehabilitation Somatic Deficits Prevail While Anxiety Plays a Minor Role Compared to Young and Middle Aged Patients
- PMID: 30425637
- PMCID: PMC6218593
- DOI: 10.3389/fnagi.2018.00345
In Older Patients Treated for Dizziness and Vertigo in Multimodal Rehabilitation Somatic Deficits Prevail While Anxiety Plays a Minor Role Compared to Young and Middle Aged Patients
Abstract
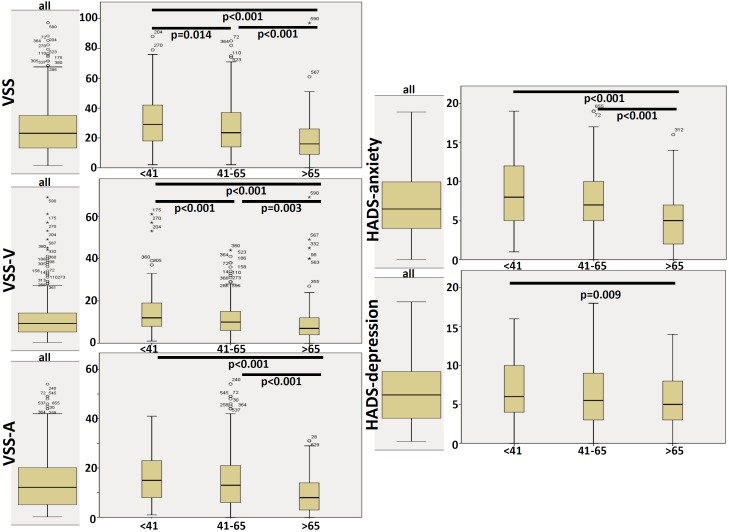
Objective: Many patients with dizziness and vertigo are of older age. It is still unclear which age-associated factors play a role in the treatment of dizziness and vertigo. Therefore, age-associated characteristics of patients subjected to an interdisciplinary day care approach for chronic vertigo and dizziness were analyzed. Subjects and Methods: 650 patients with chronic dizziness/vertigo subjected to a multimodal vestibular rehabilitation day care program were analyzed. Information concerning age, gender, medical diagnosis, medical consultations, technical diagnostics performed and therapy achieved before attending the clinic were collected. Furthermore, data were gathered using the Vertigo Severity Scale (VSS), Hospital Anxiety and Depression Scale (HADS), Mobility Inventory (MI), as well as the intensity of and the distress due to vertigo/dizziness using visual analog scales. As a follow-up, the VSS, HADS, MI, and the visual analog scales were collected again 6 months after attending the therapy program. Three age groups were compared to each other (<41, 41-65, and >65 years of age). Results: One-third of the patients were older than 65 years. This group had typical diagnoses with mainly organic deficits. In contrast to the dominance of mainly multifactorial, organic deficits the older patients reported less medical consultations, fewer technical diagnostics and even fewer treatments than the younger patients. The elderly scored significantly lower in total VSS, in VSS-V (vestibular-balance subscale), in VSS-A (autonomic-anxiety subscale) and in HADS-anxiety. Psychological diagnoses were clearly associated to the younger patients. 424 patients (65.2%) completed the follow-up questionnaire 6 months after attending the therapy week. The older patients revealed improvements of VSS-V and the Avoidance Alone scale of MI as well as decreased distress due to vertigo/dizziness. Conclusion: In the older patients, who took part in our vestibular rehabilitation program, mainly somatic deficits prevail while anxiety plays a minor role compared to young and middle aged patients. Older patients profited from vestibular rehabilitation especially in mobility and vestibular-balance. Therefore, vestibular rehabilitation programs for the elderly with a focus on physio- and occupational therapeutic interventions and less cognitive behavioral therapy may be reasonable.
Keywords: day care; dizziness; interdisciplinary; multimodal treatment; older age; vertigo.
Figures




References
-
- Aggarwal N. T., Bennett D. A., Bienias J. L., Mendes de Leon C. F., Morris M. C., Evans D. A. (2000). The prevalence of dizziness and its association with functional disability in a biracial community population. J. Gerontol. A Biol. Sci. Med. Sci. 55 M288–M292. 10.1093/gerona/55.5.M288 - DOI - PubMed
-
- Andersson E. (1993). The hospital anxiety and depression scale: homogeneity of the subscales. Soc. Behav. Person. 21 197–204. 10.2224/sbp.1993.21.3.197 - DOI
LinkOut - more resources
Full Text Sources
Research Materials