

Two cases of radiation-associated angiosarcoma of the breast
- PMID: 30426313
- PMCID: PMC6233252
- DOI: 10.1186/s40792-018-0539-8
Two cases of radiation-associated angiosarcoma of the breast
Abstract
Background: The incidence of radiation-associated angiosarcoma (RAA) of the breast has been increasing, and its prognosis is reportedly poor. It is important to remove tumor tissues completely to prevent recurrence.
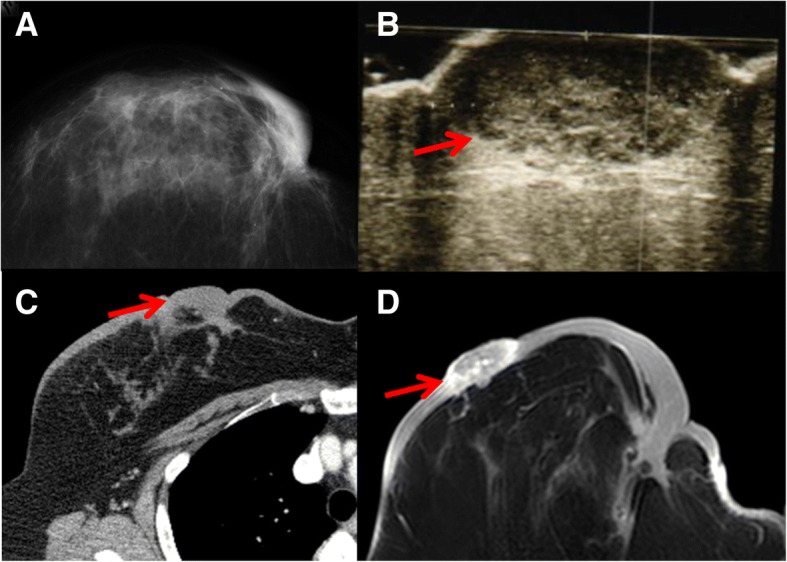
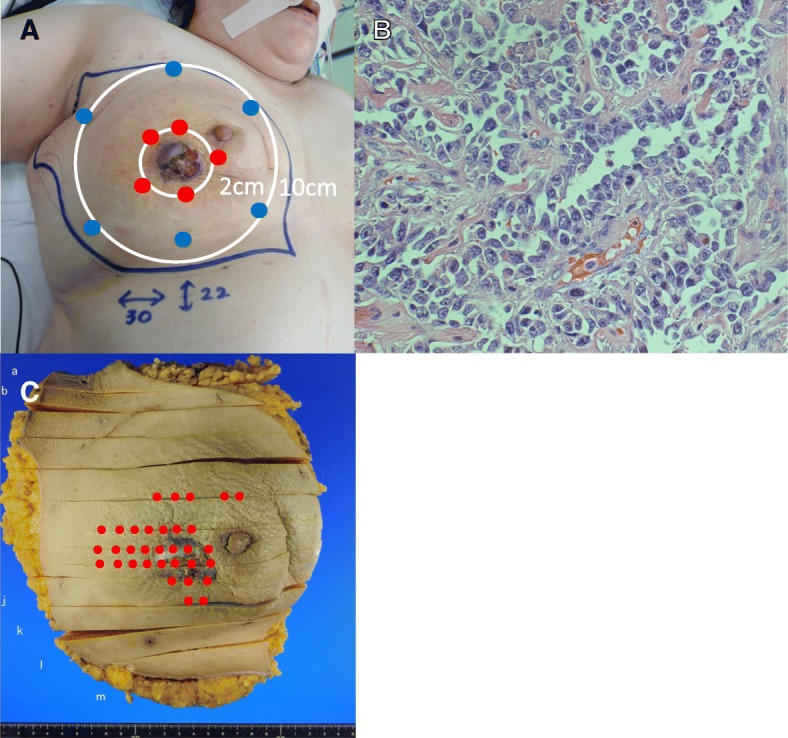
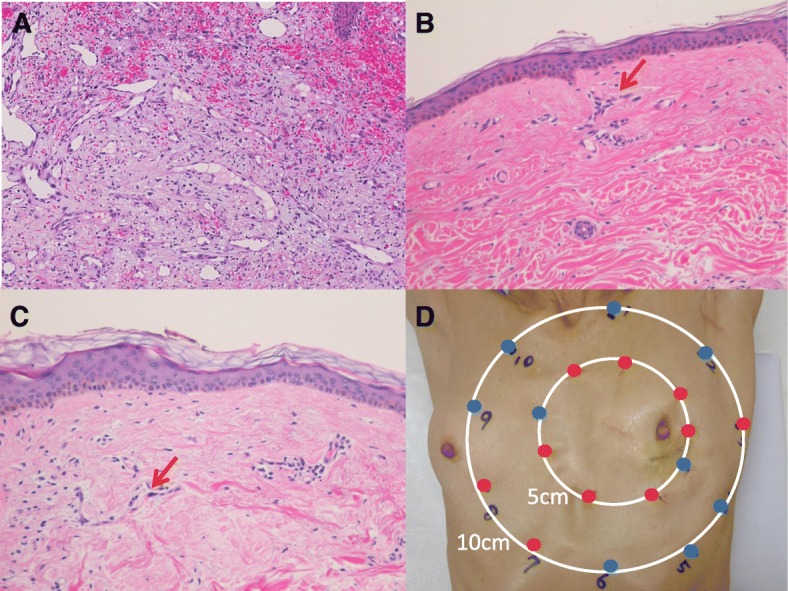
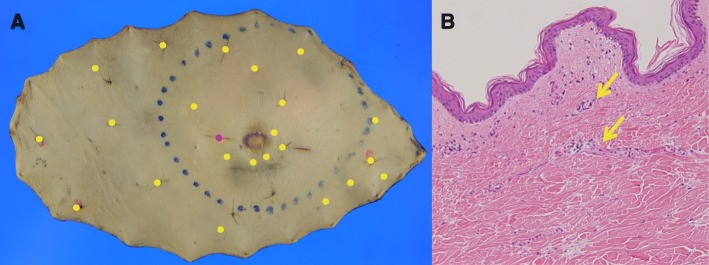
Case presentation: We report two cases of patients with RAA of the breast. Both patients had a nodule in their remaining breast a few years after undergoing breast-conserving surgery and radiation therapy for breast cancer. The nodules were diagnosed as angiosarcoma by skin biopsy and open biopsy, respectively. To determine the extent of lesion spread, mapping biopsy was performed before surgery. Both patients underwent mastectomy, extensive skin resection, and split skin grafting. Pathological findings showed that their tumors could be completely resected. After surgery, chemotherapy was performed.
Conclusion: In our cases, no local or distant recurrence has been detected in either patient for over 4 years. We identified the range of tumor invasion by preoperative mapping biopsy and completely resected all tumor tissue.
Keywords: Angiosarcoma; Breast cancer; Breast-conserving treatment; Radiation therapy; Secondary angiosarcoma.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
LinkOut - more resources
Full Text Sources
