

TRUS-guided drainage of the ectopic ureter entering the prostatic urethra and TRUS-guided transurethral neo-orifice formation using holmium laser
- PMID: 30427132
- PMCID: PMC6442213
- DOI: 10.15557/JoU.2018.0037
TRUS-guided drainage of the ectopic ureter entering the prostatic urethra and TRUS-guided transurethral neo-orifice formation using holmium laser
Abstract
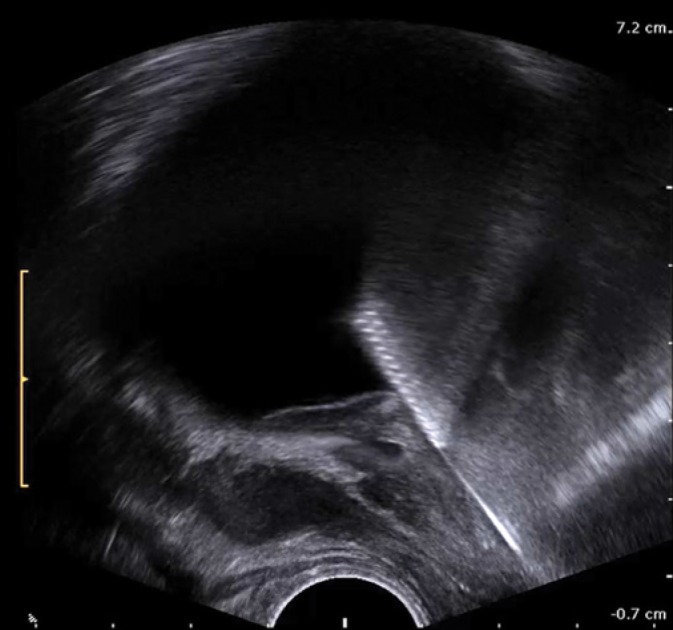
A fifty-nine year-old male was hospitalized for exacerbation of chronic pancreatitis. As a gigantic cyst of the pancreatic tail was identified, it was fused with the jejunal loop. Due to persistent fever and severe symptoms in the storage and voiding phases, the patient was referred to a urologist. Because transrectal ultrasound examination revealed a fluid collection resembling the left seminal vesicle filled with purulent material, a transrectal puncture procedure was performed. The analysis of computed tomography scans led to the diagnosis of duplicated collecting system of the left kidney with the enormous ureter of the upper moiety that entered the prostate gland. In order to permanently decompress the hydronephrosed upper moiety of the left kidney, the patient was deemed eligible for endoscopic treatment. A transurethral incision through the bladder wall and the adjacent segment of the ectopic ureter was made with holmium laser under transrectal ultrasonography guidance, thus creating a neo-orifice of this ureter.
Keywords: TRUS; ectopic ureter; holmium laser; neo-orifice; pancreatic cyst.
© Polish Ultrasound Society.
Conflict of interest statement
Authors do not report any financial or personal connections with other persons or organizations, which might negatively affect the contents of this publication and/or claim authorship rights to this publication.
Figures

















Similar articles
-
Minimally invasive transurethral laser incision for management of ectopic ureter orifice stenosis in adult patient.Urol Case Rep. 2020 Dec 22;35:101540. doi: 10.1016/j.eucr.2020.101540. eCollection 2021 Mar. Urol Case Rep. 2020. PMID: 33391992 Free PMC article.
-
Double trouble: A unique case of TRUS biopsy induced left upper moiety infection of a duplicated ectopic ureter.Urol Case Rep. 2019 Aug 13;27:100999. doi: 10.1016/j.eucr.2019.100999. eCollection 2019 Nov. Urol Case Rep. 2019. PMID: 31463201 Free PMC article.
-
Holmium:YAG transurethral incision versus laser photoselective vaporization for benign prostatic hyperplasia in a small prostate.J Urol. 2014 Jan;191(1):148-54. doi: 10.1016/j.juro.2013.06.113. Epub 2013 Jul 8. J Urol. 2014. PMID: 23845460
-
[A case of ectopic ureterocele in a male adult found during examination of a traumatic injury].Hinyokika Kiyo. 2004 Apr;50(4):245-8. Hinyokika Kiyo. 2004. PMID: 15188616 Review. Japanese.
-
Clinical Significance of Prostatic Calculi: A Review.World J Mens Health. 2018 Jan;36(1):15-21. doi: 10.5534/wjmh.17018. Epub 2017 Sep 25. World J Mens Health. 2018. PMID: 29076299 Free PMC article. Review.
References
-
- Amatulle P, Kane RA, Bradley F: Ureteral duplication anomaly with ectopic intraprostatic insertion. J Ultrasound Med 1997; 16: 231–233. - PubMed
-
- Fannin O, Cammack JT, Crotty KL, Neal DE Jr: Bilateral single ectopic ureters: Diagnosis using transrectal ultrasound. J Urol 1993; 150: 1229–1231. - PubMed
-
- Kim B, Kawashima A, Ryu JA, Takahashi N, Hartman RP, King BF Jr: Imaging of the seminal vesicle and vas deferens. Radiographics 2009; 29: 1105–1121. - PubMed
-
- Kuligowska E, Keller E, Ferrucci JT: Treatment of pelvic abscesses: Value of one-step sonographically guided transrectal needle aspiration and lavage. AJR Am J Roentgenol 1995; 164: 201–206. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials