

Evaluation of the Short-, Mid-, and Long-Term Effects of Tofacitinib on Lymphocytes in Patients With Rheumatoid Arthritis
- PMID: 30427585
- PMCID: PMC6593802
- DOI: 10.1002/art.40780
Evaluation of the Short-, Mid-, and Long-Term Effects of Tofacitinib on Lymphocytes in Patients With Rheumatoid Arthritis
Abstract
Objective: Tofacitinib is an oral JAK inhibitor for the treatment of rheumatoid arthritis (RA). Altered lymphocyte cell counts and a potential association with increased infection rates have been reported in RA patients treated with JAK inhibitors. This analysis was undertaken to evaluate the short-, mid-, and long-term effects of tofacitinib on lymphocytes and infection rates in patients with RA.
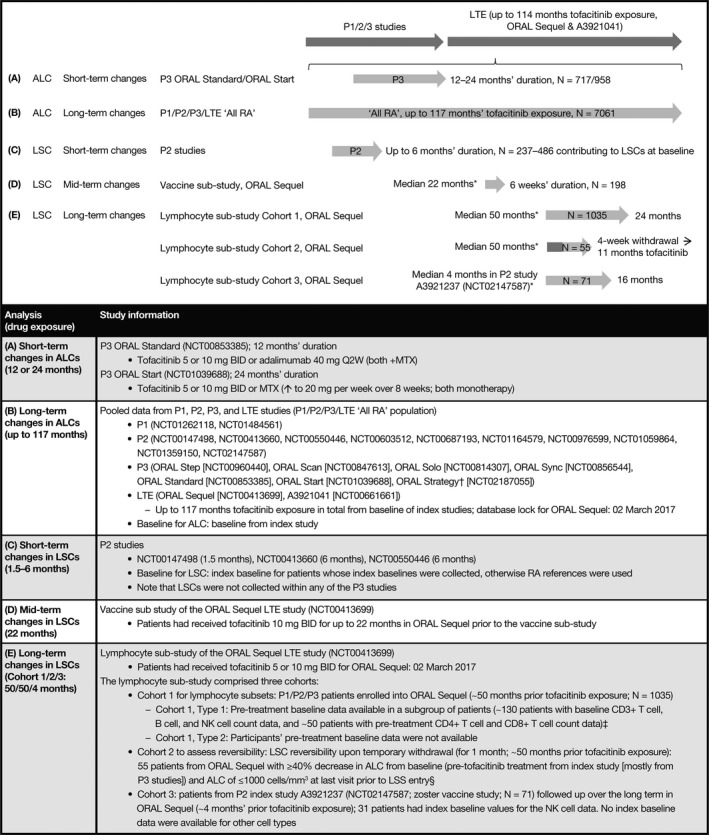
Methods: In this post hoc analysis, absolute lymphocyte counts (ALCs) were obtained from phase III studies (12-24 months; n = 717-958) and phase I/II/III/long-term extension studies of tofacitinib (≤117 months) (All RA population; n = 7,061); lymphocyte subset counts (LSCs) were from phase II studies (1.5-6 months' exposure; n = 236-486), an ORAL Sequel vaccine substudy (~22 months; n = 198), and an ORAL Sequel lymphocyte substudy (~50 months; n = 55-1,035) of tofacitinib. The reversibility of ALC/LSC changes was evaluated. The relationship of ALC and LSC to infections was analyzed in the All RA population. The value of monitoring ALC alone was assessed by examining correlations between ALCs and LSCs.
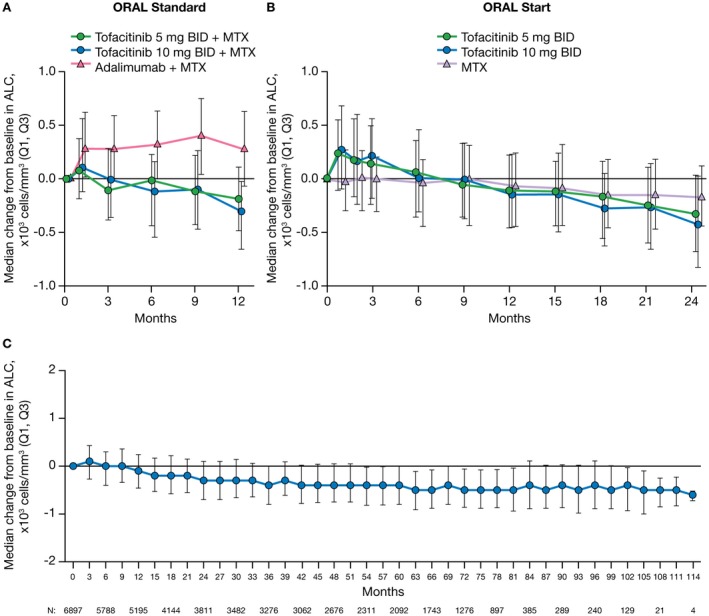
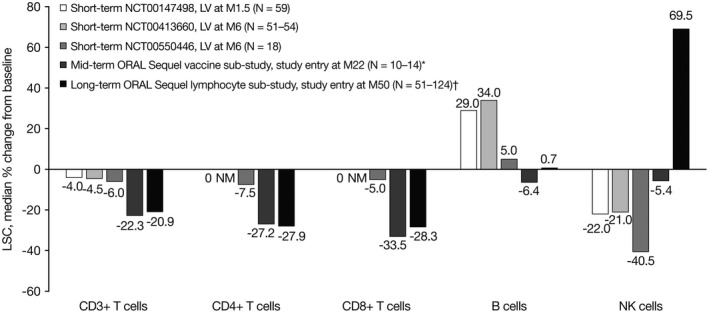
Results: Tofacitinib treatment resulted in an initial increase in ALC versus pretreatment baseline, which gradually declined to steady state by ~48 months. CD4+ and CD8+ T cell counts decreased over long-term treatment, and ALC and LSC changes were reversible upon treatment cessation. Patients with ALCs of <500 cells/mm3 had an increased risk of serious infections. There was no strong association between CD4+ T cell, CD8+ T cell, B cell, or natural killer cell counts and serious infection incidence rates. ALC and CD4+ or CD8+ T cell counts correlated well (R = 0.65-0.86).
Conclusion: Our findings indicate that monitoring of ALC alone appears to be adequate to assess infection risk in tofacitinib-treated patients with RA.
© 2018 Pfizer Inc. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
References
-
- Fleischmann R, Cutolo M, Genovese MC, Lee EB, Kanik KS, Sadis S, et al. Phase IIb dose‐ranging study of the oral JAK inhibitor tofacitinib (CP‐690,550) or adalimumab monotherapy versus placebo in patients with active rheumatoid arthritis with an inadequate response to disease‐modifying antirheumatic drugs. Arthritis Rheum 2012;64:617–29. - PubMed
-
- Kremer JM, Bloom BJ, Breedveld FC, Coombs JH, Fletcher MP, Gruben D, et al. The safety and efficacy of a JAK inhibitor in patients with active rheumatoid arthritis: results of a double‐blind, placebo‐controlled phase IIa trial of three dosage levels of CP‐690,550 versus placebo. Arthritis Rheum 2009;60:1895–905. - PubMed
-
- Kremer JM, Cohen S, Wilkinson BE, Connell CA, French JL, Gomez‐Reino J, et al. A phase IIb dose‐ranging study of the oral JAK inhibitor tofacitinib (CP‐690,550) versus placebo in combination with background methotrexate in patients with active rheumatoid arthritis and an inadequate response to methotrexate alone. Arthritis Rheum 2012;64:970–81. - PubMed
-
- Tanaka Y, Suzuki M, Nakamura H, Toyoizumi S, Zwillich SH, Tofacitinib Study Investigators . Phase II study of tofacitinib (CP‐690,550) combined with methotrexate in patients with rheumatoid arthritis and an inadequate response to methotrexate. Arthritis Care Res (Hoboken) 2011;63:1150–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
