

The coronary circulation in acute myocardial ischaemia/reperfusion injury: a target for cardioprotection
- PMID: 30428011
- PMCID: PMC6529918
- DOI: 10.1093/cvr/cvy286
The coronary circulation in acute myocardial ischaemia/reperfusion injury: a target for cardioprotection
Abstract
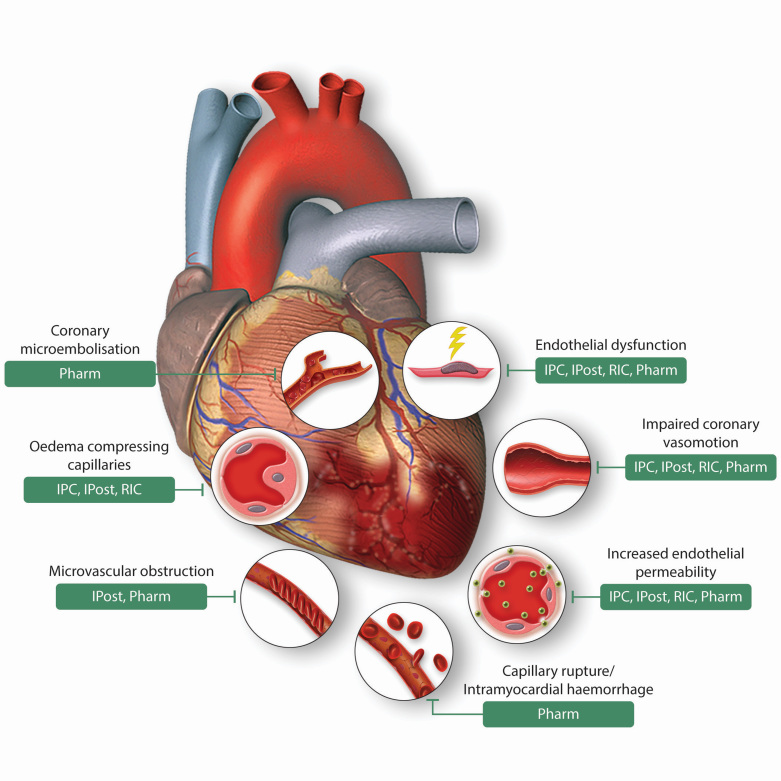
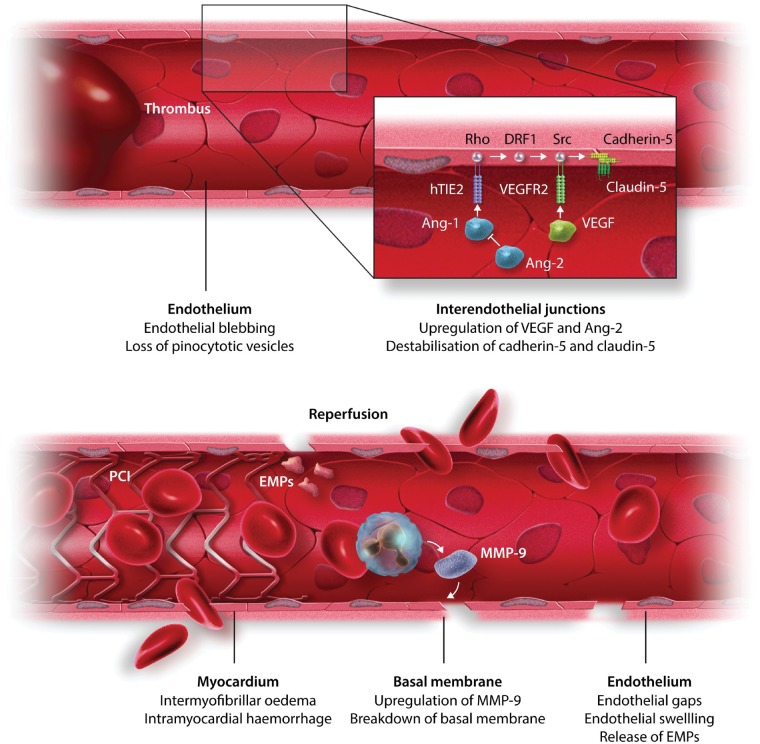
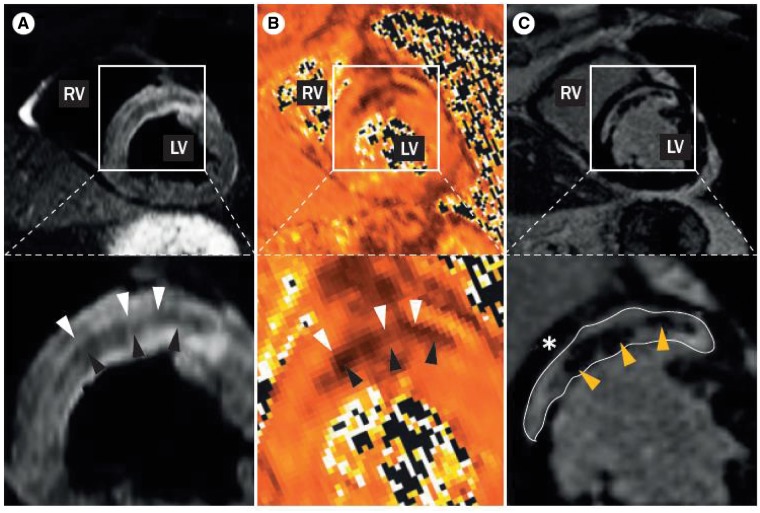
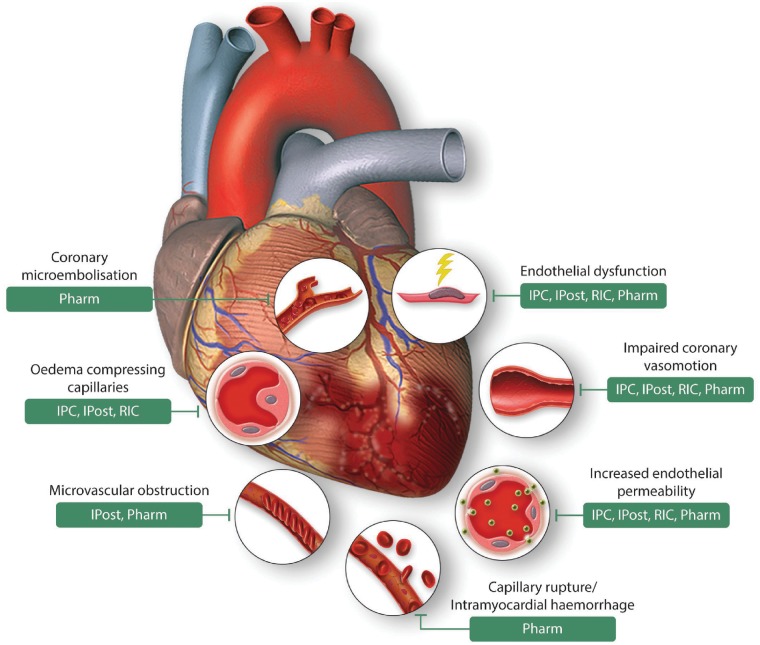
The coronary circulation is both culprit and victim of acute myocardial infarction. The rupture of an epicardial atherosclerotic plaque with superimposed thrombosis causes coronary occlusion, and this occlusion must be removed to induce reperfusion. However, ischaemia and reperfusion cause damage not only in cardiomyocytes but also in the coronary circulation, including microembolization of debris and release of soluble factors from the culprit lesion, impairment of endothelial integrity with subsequently increased permeability and oedema formation, platelet activation and leucocyte adherence, erythrocyte stasis, a shift from vasodilation to vasoconstriction, and ultimately structural damage to the capillaries with eventual no-reflow, microvascular obstruction (MVO), and intramyocardial haemorrhage (IMH). Therefore, the coronary circulation is a valid target for cardioprotection, beyond protection of the cardiomyocyte. Virtually all of the above deleterious endpoints have been demonstrated to be favourably influenced by one or the other mechanical or pharmacological cardioprotective intervention. However, no-reflow is still a serious complication of reperfused myocardial infarction and carries, independently from infarct size, an unfavourable prognosis. MVO and IMH can be diagnosed by modern imaging technologies, but still await an effective therapy. The current review provides an overview of strategies to protect the coronary circulation from acute myocardial ischaemia/reperfusion injury. This article is part of a Cardiovascular Research Spotlight Issue entitled 'Cardioprotection Beyond the Cardiomyocyte', and emerged as part of the discussions of the European Union (EU)-CARDIOPROTECTION Cooperation in Science and Technology (COST) Action, CA16225.
Keywords: Cardioprotection; Coronary circulation; Ischaemia; Microvascular obstruction; Reperfusion.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2018. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Yellon DM, Hausenloy DJ.. Myocardial reperfusion injury. N Engl J Med 2007;357:1121–1135. - PubMed
-
- Ibanez B, Heusch G, Ovize M, Van de Werf F.. Evolving therapies for myocardial ischemia/reperfusion injury. J Am Coll Cardiol 2015;65:1454–1471. - PubMed
-
- Kleinbongard P, Amanakis G, Skyschally A, Heusch G.. Reflection of cardioprotection by remote ischemic perconditioning in attenuated ST-segment elevation during ongoing coronary occlusion in pigs: evidence for cardioprotection from ischemic injury. Circ Res 2018;122:1102–1108. - PubMed
-
- Heusch G, Gersh BJ.. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. Eur Heart J 2017;38:774–784. - PubMed
