

Comparative effectiveness of anti-viral drugs with dual activity for treating hepatitis B and HIV co-infected patients: a network meta-analysis
- PMID: 30428847
- PMCID: PMC6234602
- DOI: 10.1186/s12879-018-3506-x
Comparative effectiveness of anti-viral drugs with dual activity for treating hepatitis B and HIV co-infected patients: a network meta-analysis
Abstract
Background: There are randomized trials assessing a variety of antiviral drugs for hepatitis B virus (HBV), but the relative effectiveness of these drugs in the treatment of patients co-infected with human immunodeficiency virus (HIV) remains unclear. The objectives of the current study were to estimate and rank the relative effectiveness of antiviral drugs for treating HBV and HIV co-infected patients.
Methods: Randomized trials, assessing the efficacy of antiviral drugs for HBV and HIV co-infected patients were searched in health-related databases. The methodological quality of the included trials was evaluated using the Cochrane risk of bias tool. Main outcome in this meta-analysis study was the success of treatment by antivirals as determined by virologic response. We performed pairwise and network meta-analysis of these trials and assessed the quality of evidence using the GRADE approach.
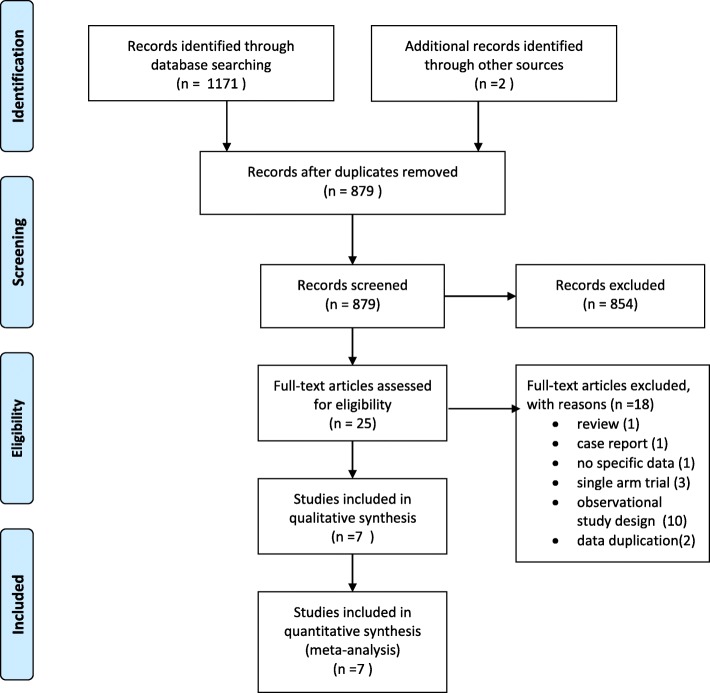
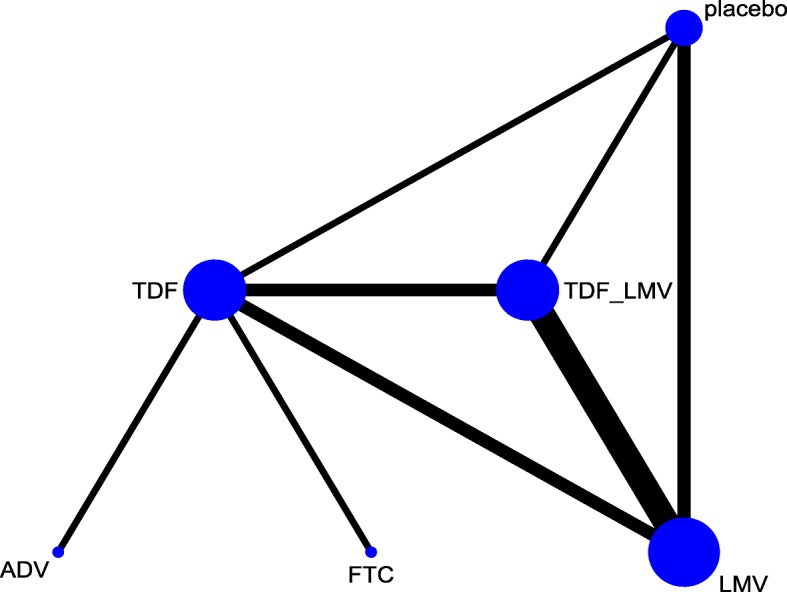
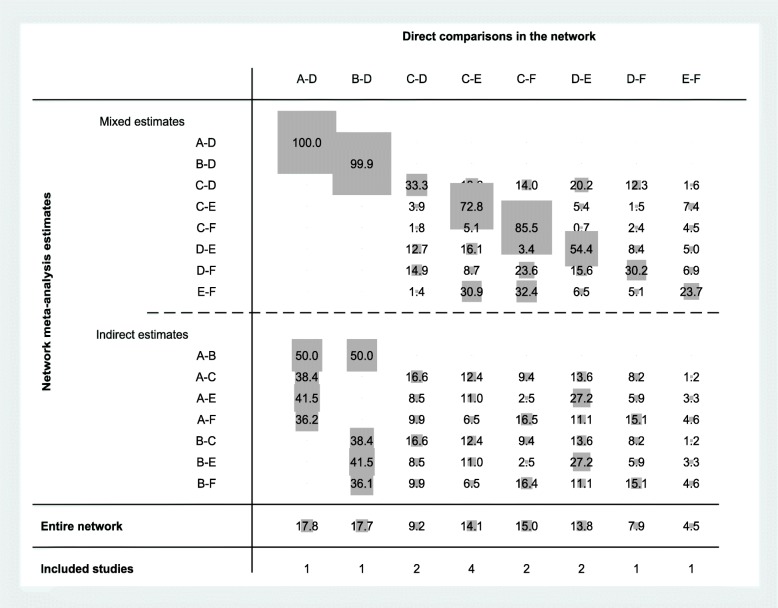
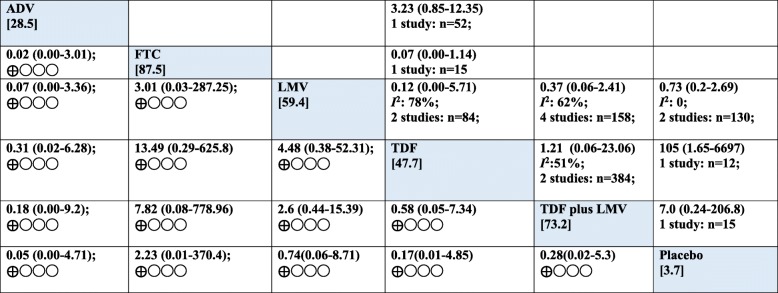
Results: Seven randomized trials (329 participants) were included in this network meta-analysis study. A network geometry was formed with six treatment options including four antiviral drugs, adefovir (ADV), emtricitabine (FTC), lamivudine (LMV) and tenofovir disoproxil fumarate (TDF), combination treatment of TDF plus LMV, and placebo. The weighted percentage contributions of each comparison distributed fairly equally in the entire network of evidence. An assumption of consistency required for network meta-analysis was not violated (the global Wald test for inconsistency: Chi2(4) = 3.63, p = 0.46). The results of estimates showed no differences between the treatment regimens in terms of viral response for treating HBV and HIV co-infected patients, which spanned both benefit and harm (e.g. LMV vs TDF plus LMV: OR: 0.37, 95%CI: 0.06-2.41). Overall, the certainty of evidence was very low in all comparisons (e.g. LMV vs TDF plus LMV: 218 fewer per 1000,121 more to 602 fewer, very low certainty). Therefore, we remained uncertain to the true ranking of the antiviral treatments in HBV/ HIV co-infected patients.
Conclusions: The findings suggest that the evidence is insufficient to provide guidance to the relative effectiveness of currently available antiviral drugs with dual activity in treating co-infection of HBV/HIV. Well-designed, large clinical trials in this field to address other important outcomes from different epidemiological settings are recommended.
Keywords: Antiviral; HIV; Hepatitis B; Network meta-analysis.
Conflict of interest statement
Ethics approval and consent to participate
The need for approval was waived as this study solely used published human data.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Konopnicki D, Mocroft A, de Wit S, Antunes F, Ledergerber B, Katlama C, et al. Hepatitis B and HIV: prevalence, AIDS progression, response to highly active antiretroviral therapy and increased mortality in the EuroSIDA cohort. AIDS. 2005;19:593–601. doi: 10.1097/01.aids.0000163936.99401.fe. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
