

An Unusual Case of Intestinal Malrotation Causing Duodenal Obstruction by a Looped Appendix
- PMID: 30429450
- PMCID: PMC6250999
- DOI: 10.12659/AJCR.913039
An Unusual Case of Intestinal Malrotation Causing Duodenal Obstruction by a Looped Appendix
Abstract
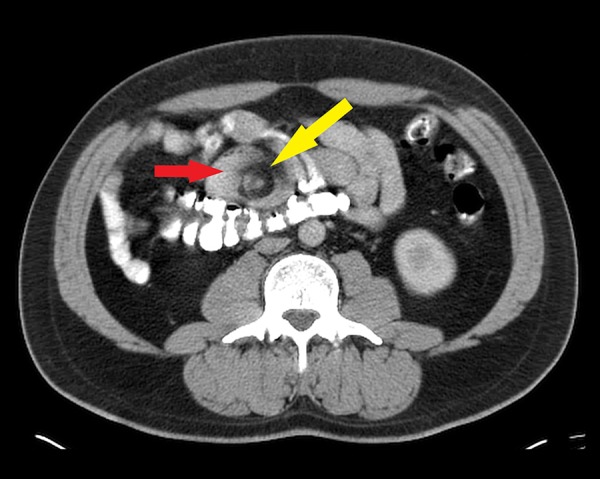
BACKGROUND Bowel obstruction is a mechanical or functional obstruction of the intestines which prevents the normal movement of the products of digestion. Intestinal malrotation is one of the rarest causes of mechanical bowel obstruction. In adults, the incidence rate is 0.2%, and 15% of all patients with confirmed diagnosis remain asymptomatic throughout life. Surgery is generally required when the patient is symptomatic. CASE REPORT A 30-year-old man with multiple admissions for chronic intermittent colicky abdominal pain since childhood, was admitted for symptoms suggestive of proximal small bowel obstruction. Tomographic imaging identified a midgut malrotation and a duodenal obstruction by a non-diseased displaced appendix. Laparoscopic liberation of the duodenum and the terminal ilium was done successfully. CONCLUSIONS Intestinal malrotation is infrequently encountered in the adult population, but it should be kept in mind as a differential diagnosis whenever a case of acute intestinal obstruction in an adult presents without any significant past surgical history.
Conflict of interest statement
None.
Figures





References
-
- Gamblin TC, Stephens RE, Jr, Johnson RK, et al. Adult malrotation: A case report and review of the literature. Curr Surg. 2003;60(5):517–20. - PubMed
-
- Vukie Z. Presentation of intestinal malrotation syndromes in older children and adults: Report of three cases. Croat Med J. 1998;39(4):455–57. - PubMed
-
- Maxon RT, Franklin PA, Wagner CW. Malrotation in the older child: Surgical management treatment and outcome. Am Surg. 1995;61(2):135–38. - PubMed
-
- Dietz DW, Walsh RM, Grudfest-Broniatowski S, et al. Intestinal malrotation: Rare but important cause of bowel obstruction in adults. Dis Colon Rectum. 2002;45(10):1381–86. - PubMed
-
- Kapfer S, Rappold J. Intestinal malrotation not just the pediatric surgeon’s problem. J Am Coll Surg. 2004;199:628–35. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
