

Conservative treatment of fingertip injuries in children - first experiences with a novel silicone finger cap that enables woundfluid analysis
- PMID: 30430061
- PMCID: PMC6218674
- DOI: 10.3205/iprs000125
Conservative treatment of fingertip injuries in children - first experiences with a novel silicone finger cap that enables woundfluid analysis
Abstract
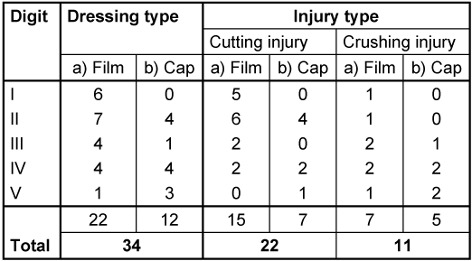
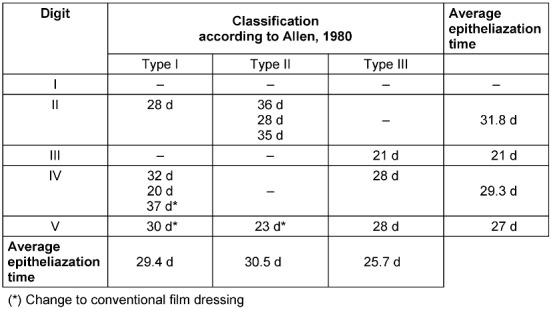
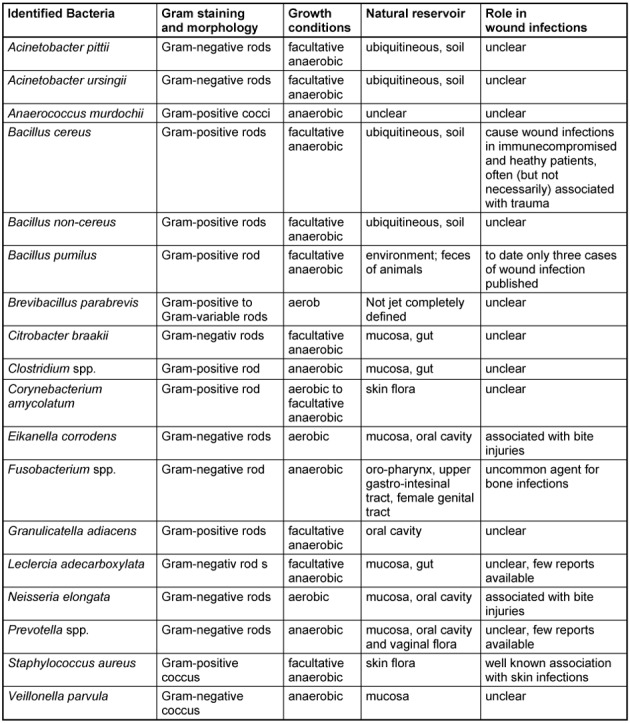
Introduction: Human fingertips are able to regenerate soft tissue and skin after amputation injuries with excellent cosmetic and functional results when treated with semiocclusive dressings. Despite bacterial colonizations, proceeding infections are not reported with this management. The underlying mechanisms for this form of regenerative healing as well as for the resilience to infections are not known. Due to the lack of mechanical protection, the leakage of maloderous woundfluid and the sometimes challenging application, conventional film dressings have their problems, especially in treating young children. We therefore treated selected patients with a novel silicone finger cap with an integrated wound fluid reservoir that enables atraumatic routine wound fluid aspiration. Methods: We report on 34 patients in between 1 and 13 years with traumatic fingertip amputations primarily treated with occlusive dressings. 12 patients were treated with a novel silicone finger cap. We summarized clinical data for each patient. This included photographs and microbiological results from wound fluid analyses, whenever available. Results: The results of both, conventional film dressing and silicone finger cap treatment, were excellent with no hypersensitivity and no restrictions in sensibility and motility. Even larger pulp defects were rearranged in a round shape and good soft tissue coverage of the distal phalanx was achieved. Nail deformities were not observed. We detected a wide spectrum of both aerobic and anaerobic bacteria in the wound fluids but infections were not observed. Epithelialization times did not differ significantly and no severe complications were seen in all primarily conservatively treated patients. Conclusion: This study provides preliminary data demonstrating that the treatment with the silicone finger cap leads to excellent clinical results in wound healing. Interestingly, the wounds were colonized with a wide range of bacteria including species that may cause wound infections. However, we saw no proceeding inflammation and the regeneration was undisturbed. In the future, the efficacy of this new management should be evaluated in randomized, controlled clinical trials to confirm the results under standard conditions and get more insight into the role of the wound microbiome as well as other factors that may promote regeneration. The aspirable Reservoir of the finger cap will enable easy atraumatic sampling of wound fluids both for diagnostic and for research purposes as well as possibly allowing direct administration of pro-regenerative drugs in the future.
Einleitung: Fingerendglieder können nach Amputationsverletzungen mit hervorragenden kosmetischen und funktionellen Ergebnissen regenerieren, wenn die Verletzungen mit semiokklusiven Verbänden behandelt werden. Trotz der bakteriellen Kolonisation dieser Wunden werden keine fortschreitenden Infektionen berichtet. Der Mechanismus für diese regenerative Heilung und die Resilienz gegen Infektionen ist unbekannt. Aufgrund der Leckage von übelriechender Wundflüssigkeit und wegen des Fehlens eines mechanischen Schutzes sowie durch die mitunter schwierige Anlage selbstklebender Folien, sind diese bei der Versorgung von Kindern teilweise problematisch. Daher behandelten wir ausgewählte Patienten mit individuell gefertigten Silikonfingerlingen. Dabei wurde regelmäßig Wundflüssigkeit aus einem integrierten Reservoir aspiriert und bakteriologisch untersucht.Material und Methoden: Wir berichten über 34 Patienten zwischen 1 und 13 Jahren mit traumatischen Fingerendgliedteilamputationen, welche primär semiokklusiv behandelt wurden. 12 Patienten wurden dabei mit dem neuartigen Fingerling behandelt. Wir werteten retrospektiv die Patientenakten aus. Dies beinhaltet Fotodokumentationen und mikrobiologische Untersuchungsergebnisse wenn vorhanden. Ergebnisse: Die Ergebnisse beider Behandlungsverfahren waren sehr gut: Es gab weder Sensibilitätsstörungen noch Bewegungseinschränkungen. Auch nach größeren Weichteildefekten resultierten kosmetisch schöne Fingerkuppen mit guter Weichteildeckung der distalen Phalanx. Nageldeformitäten wurden nicht festgestellt. In den bakteriologischen Untersuchungen der Wundflüssigkeiten fand sich ein großes Spektrum an aeroben und anaeroben Keimen. Fortschreitende Infektionen gab es nicht. Die Heilungszeiten waren vergleichbar bei beiden Behandlungsformen. In den primär konservativ behandelten Patienten wurden keine ernsten Komplikationen festgestellt.Conclusio: Fingerendgliedteilamputationen bei Kindern können grundsätzlich erfolgreich konservativ mit dem neuen Silikonfingerling behandelt werden. Die Wunden sind dabei mit Bakterien kolonisiert. Dabei sind auch als Erreger von Wundinfektionen bekannte Keime. Dennoch kam es nicht zu fortschreitenden Infektionen und die regenerative Heilung schien nicht gestört. In Zukunft bedarf es randomisierter, kontrollierter Studien, um die Wirksamkeit des Silikonfingerlings nachzuweisen und mehr über die Rolle des Mikrobioms und anderer Faktoren zu erfahren, die möglicherweise die Regeneration beeinflussen. Durch das punktierbare Wundflüssigkeitsreservoir im Silikonfingerling kann dabei Wundflüssigkeit regelmäßig für diagnostische und wissenschaftliche Zwecke entnommen werden. Weiterhin könnten in Zukunft regenerationsfördernde Substanzen auf diesem Weg atraumatisch in die Wunde eingebracht werden.
Keywords: fingertip amputation; fingertip injury; fingertip regeneration; infection; occlusive dressings; pediatric surgery; wound fluid.
Figures





Similar articles
-
Study protocol for a randomized controlled pilot-trial on the semiocclusive treatment of fingertip amputation injuries using a novel finger cap.Medicine (Baltimore). 2017 Oct;96(41):e8224. doi: 10.1097/MD.0000000000008224. Medicine (Baltimore). 2017. PMID: 29019891 Free PMC article. Clinical Trial.
-
Semi-occlusive management of fingertip injuries with finger caps: A randomized controlled trial in children and adults.Medicine (Baltimore). 2022 Jul 8;101(27):e29324. doi: 10.1097/MD.0000000000029324. Medicine (Baltimore). 2022. PMID: 35801770 Free PMC article. Clinical Trial.
-
[Outcomes of fingertip injury treatment with semi-occlusive dressings combined with surgical management within an expanded indication].Handchir Mikrochir Plast Chir. 2025 Feb;57(1):32-43. doi: 10.1055/a-2496-2706. Epub 2025 Jan 20. Handchir Mikrochir Plast Chir. 2025. PMID: 39832768 German.
-
Fingertip Injuries and Amputations: A Review of the Literature.Cureus. 2020 May 26;12(5):e8291. doi: 10.7759/cureus.8291. Cureus. 2020. PMID: 32601565 Free PMC article. Review.
-
Fingertip injuries: an update on management.J Am Acad Orthop Surg. 2013 Dec;21(12):756-66. doi: 10.5435/JAAOS-21-12-756. J Am Acad Orthop Surg. 2013. PMID: 24292932 Review.
Cited by
-
Long-term outcomes of homodigital neurovascular island flap reconstruction of fingertip injuries in children.J Hand Surg Eur Vol. 2022 Sep;47(8):845-850. doi: 10.1177/17531934221108470. Epub 2022 Jul 3. J Hand Surg Eur Vol. 2022. PMID: 35786078 Free PMC article.
-
Nail Regeneration of an Allen III Fingertip Amputation After a Dog Bite Using the Semi-occlusive Dressing Technique: A Case Report and Literature Review.Cureus. 2021 Aug 10;13(8):e17068. doi: 10.7759/cureus.17068. eCollection 2021 Aug. Cureus. 2021. PMID: 34522546 Free PMC article.
-
Local or distal flap in the management of digital trauma in children.Afr J Paediatr Surg. 2022 Jan-Mar;19(1):5-8. doi: 10.4103/ajps.AJPS_56_21. Afr J Paediatr Surg. 2022. PMID: 34916343 Free PMC article.
-
Semi-occlusive dressings for the management of fingertip amputations: A systematic review.J Hand Microsurg. 2025 Mar 1;17(3):100241. doi: 10.1016/j.jham.2025.100241. eCollection 2025 May. J Hand Microsurg. 2025. PMID: 40182737 Review.
References
-
- Damert HG, Altmann S. Behandlung von Fingerkuppenamputationen mittels Semiokklusivverband. [Treatment of fingertip amputation with semiocclusive dressing]. Unfallchirurg. 2012 Sep;115(9):798–801. doi: 10.1007/s00113-012-2258-0. doi: 10.1007/s00113-012-2258-0. (Ger). Available from: - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
