

Successful treatment of pyoderma gangrenosum with concomitant immunoglobulin A nephropathy: A case report and review of literature
- PMID: 30430129
- PMCID: PMC6232568
- DOI: 10.12998/wjcc.v6.i13.703
Successful treatment of pyoderma gangrenosum with concomitant immunoglobulin A nephropathy: A case report and review of literature
Abstract
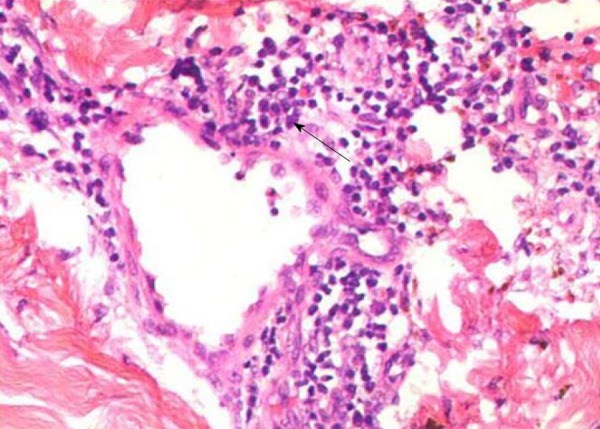
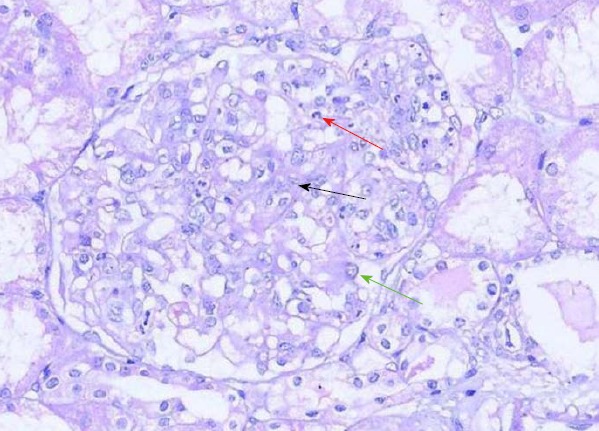
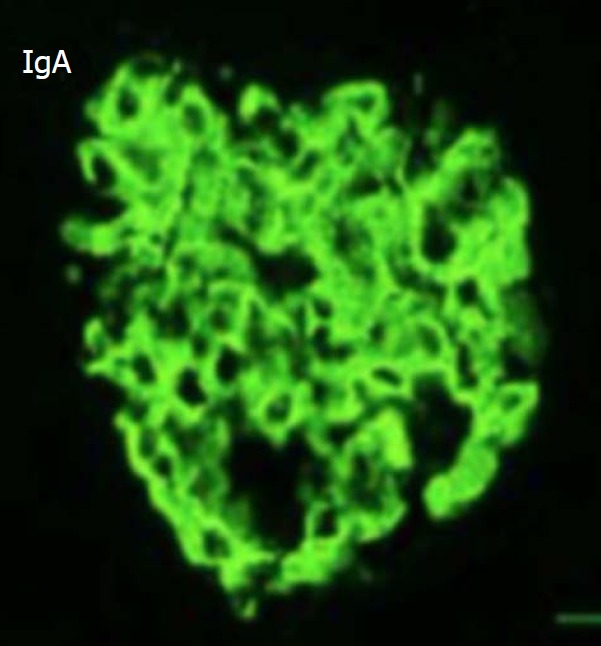
Pyoderma gangrenosum (PG) is an uncommon ulcerative cutaneous condition of an unknown etiology and is often associated with immune diseases. However, PG rarely shows visceral involvement, especially in the kidney. A 20-year-old female presented with pedal edema and skin ulceration of both lower limbs. The skin lesion began as an erythematous plaque and then became a blister. She also complained of abdominal distension and a decreasing urine volume. Laboratory data showed high proteinuria, hypoalbuminemia and hyperlipidemia. Her skin and kidney were biopsied. The pathological results indicated PG and immunoglobulin A (IgA) nephropathy. The patient was finally cured with prednisolone in combination with cyclosporine A (CsA).
Keywords: Immunoglobulin A nephropathy; Pyoderma gangrenosum; Treatment.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported.
Figures


References
-
- Ahronowitz I, Harp J, Shinkai K. Etiology and management of pyoderma gangrenosum: a comprehensive review. Am J Clin Dermatol. 2012;13:191–211. - PubMed
-
- Alavi A, French LE, Davis MD, Brassard A, Kirsner RS. Pyoderma Gangrenosum: An Update on Pathophysiology, Diagnosis and Treatment. Am J Clin Dermatol. 2017;18:355–372. - PubMed
-
- Perry HO, Brunsting LA. Pyoderma gangrenosum; a clinical study of nineteen cases. AMA Arch Derm. 1957;75:380–386. - PubMed
-
- Brown TS, Marshall GS, Callen JP. Cavitating pulmonary infiltrate in an adolescent with pyoderma gangrenosum: a rarely recognized extracutaneous manifestation of a neutrophilic dermatosis. J Am Acad Dermatol. 2000;43:108–112. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
