

Proximal pulmonary arterial wall disease in patients with persistent pulmonary hypertension after successful left-sided valve replacement according to the hemodynamic phenotype
- PMID: 30430894
- PMCID: PMC6295709
- DOI: 10.1177/2045894018816972
Proximal pulmonary arterial wall disease in patients with persistent pulmonary hypertension after successful left-sided valve replacement according to the hemodynamic phenotype
Abstract
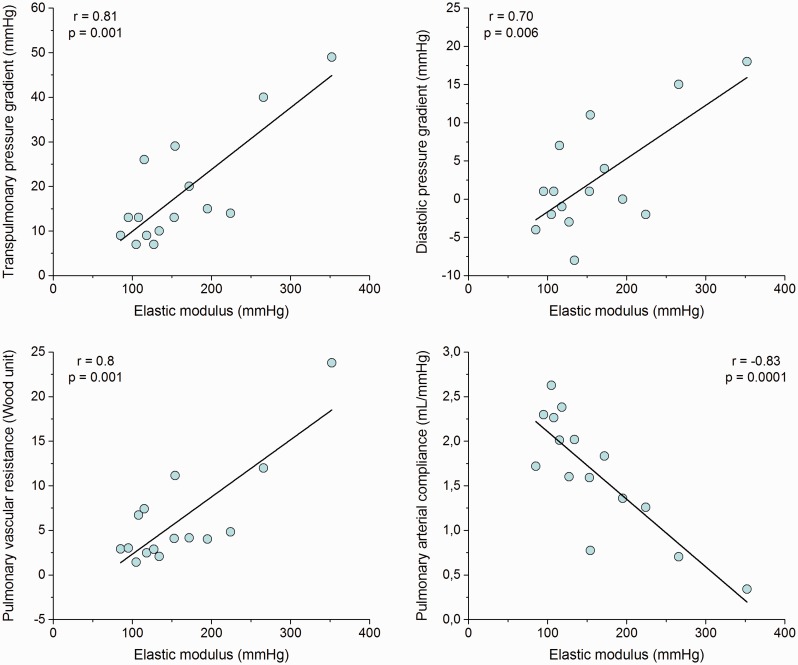
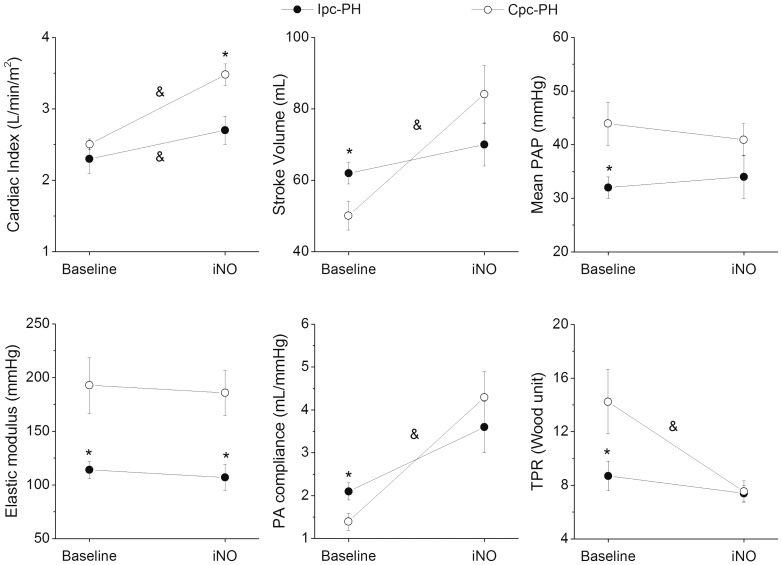
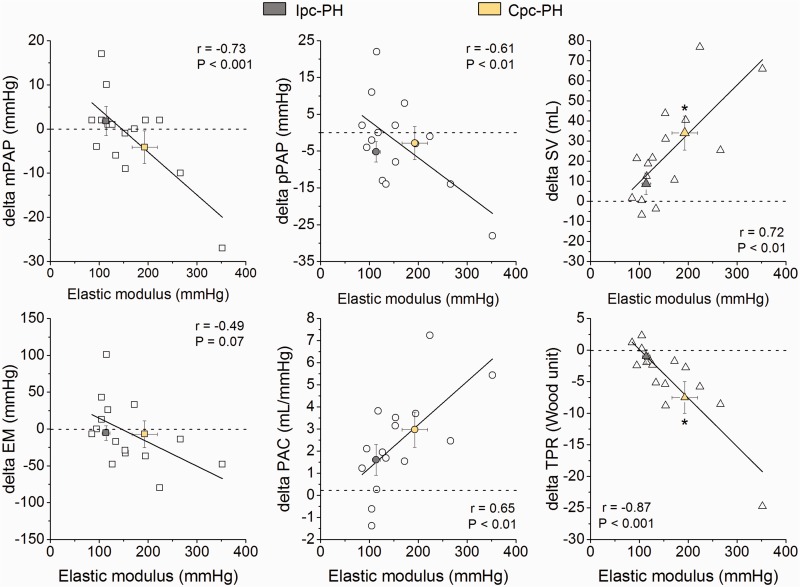
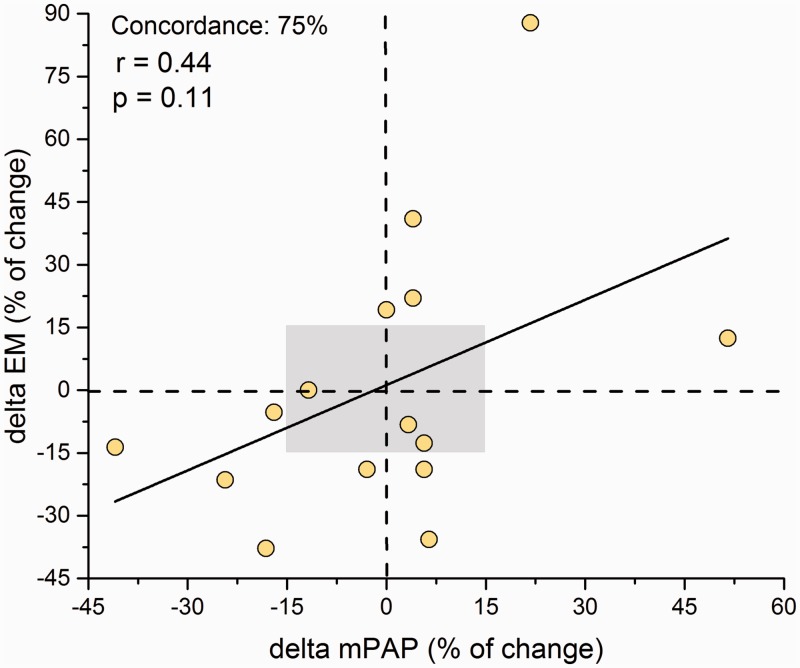
Regression of pulmonary hypertension (PH) is often incomplete after successful left-sided valve replacement (LSVR). Proximal pulmonary arterial (PPA) wall disease can be involved in patients with persistent-PH after LSVR, affecting the right ventricular to pulmonary arterial (RV-PA) coupling. Fifteen patients underwent successful LSVR at least one year ago presenting PH by echo (> 50 mmHg). Prosthesis-patient mismatch and left ventricular dysfunction were discarded. All patients underwent hemodynamic and intravascular ultrasound (IVUS) study. We estimated PPA stiffness (elastic modulus [EM]) and the relative area wall thickness (AWT). Acute vasoreactivity was assessed by inhaled nitric oxide (iNO) testing. RV-PA coupling was estimated by the tricuspid annular plane systolic excursion to systolic pulmonary arterial pressure ratio. Patients were classified as isolated post-capillary PH (Ipc-PH; pulmonary vascular resistance [PVR] ≤ 3 WU and/or diastolic pulmonary gradient [DPG] < 7 mmHg) and combined post- and pre-capillary PH (Cpc-PH; PVR > 3 WU and DPG ≥ 7 mmHg). Both Ipc-PH and Cpc-PH showed a significant increase of EM and AWT. Despite normal PVR and DPG, Ipc-PH had a significant decrease in pulmonary arterial capacitance and RV-PA coupling impairment. Cpc-PH had worse PA stiffness and RV-PA coupling to Ipc-PH ( P < 0.05). iNO decreased RV afterload, improving the cardiac index and stroke volume only in Cpc-PH ( P < 0.05). Patients with persistent PH after successful LSVR have PPA wall disease and RV-PA coupling impairment beyond the hemodynamic phenotype. Cpc-PH is responsive to iNO, having the worse PA stiffness and RV-PA coupling. The PPA remodeling could be an early event in the natural history of PH associated with left heart disease.
Keywords: inhaled nitric oxide; left-sided valve replacement; pulmonary arterial wall; pulmonary hypertension; right ventricular to pulmonary arterial coupling.
Figures
References
-
- Hoeper MM, Humbert M, Souza R, et al. A global view of pulmonary hypertension. Lancet Respir Med 2016; 4: 306–322. - PubMed
-
- Magne J, Pibarot P, Sengupta PP, et al. Pulmonary hypertension in valvular disease: A comprehensive review on pathophysiology to therapy from the HAVEC group. JACC Cardiovasc Imaging 2015; 8: 83–99. - PubMed
-
- Martinez C, Bernard A, Dulgheru R, et al. Pulmonary hypertension in aortic stenosis and mitral regurgitation: Rest and exercise echocardiography significance. Prog Cardiovasc Dis 2016; 59: 59–70. - PubMed
-
- Guazzi M, Naeije R. Pulmonary hypertension in heart failure: Pathophysiology, pathobiology, and emerging clinical perspectives. J Am Coll Cardiol 2017; 69: 1718–1734. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
