

Electrophysiological Guidance of Epidural Electrode Array Implantation over the Human Lumbosacral Spinal Cord to Enable Motor Function after Chronic Paralysis
- PMID: 30430902
- PMCID: PMC6482916
- DOI: 10.1089/neu.2018.5921
Electrophysiological Guidance of Epidural Electrode Array Implantation over the Human Lumbosacral Spinal Cord to Enable Motor Function after Chronic Paralysis
Abstract
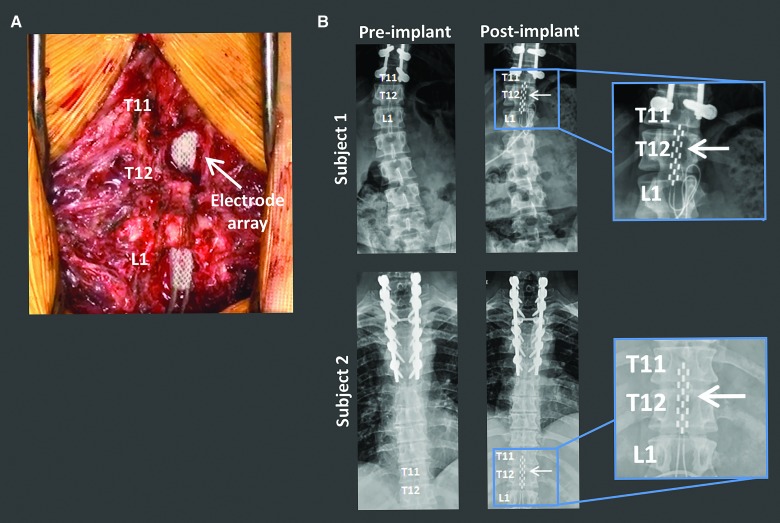
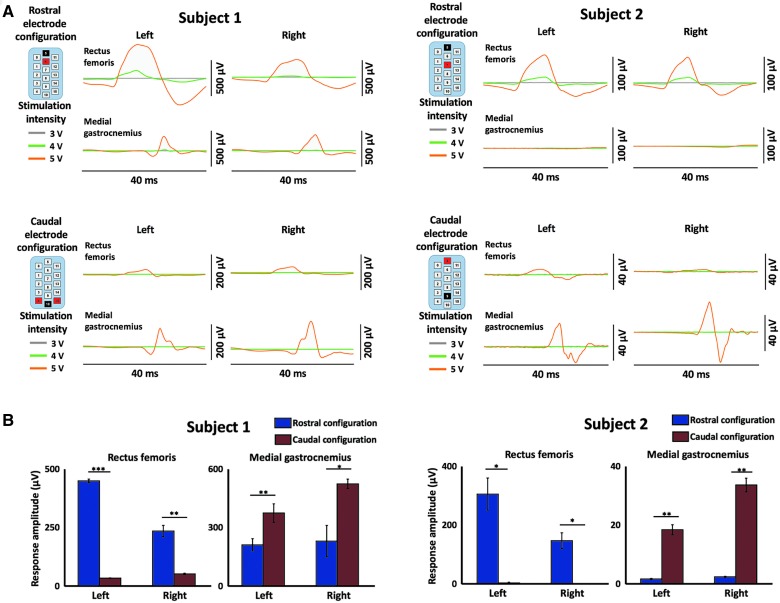
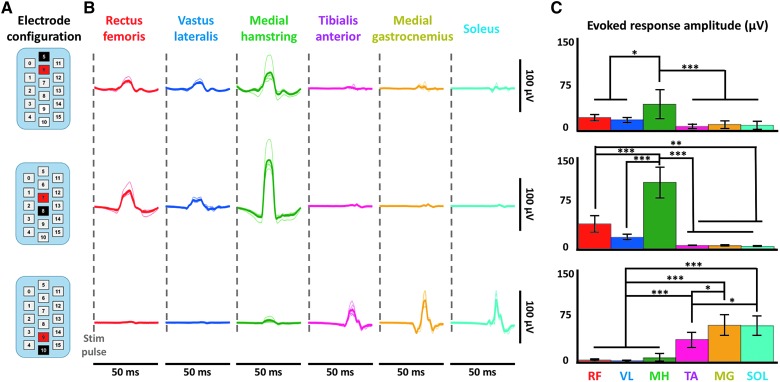
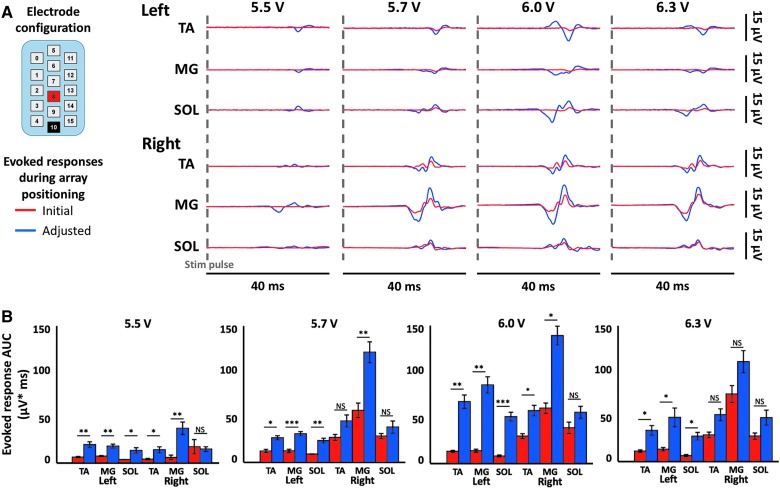
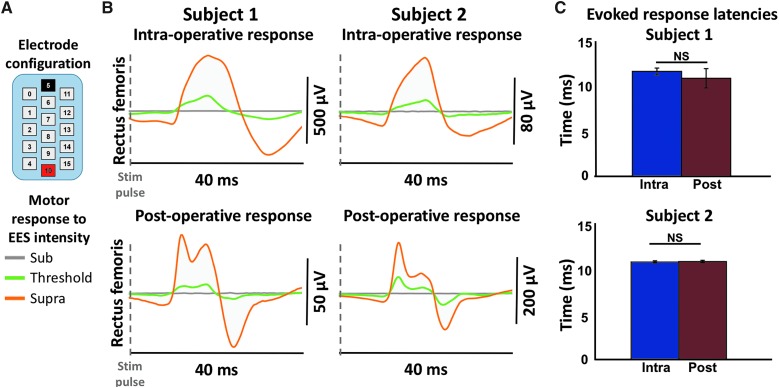
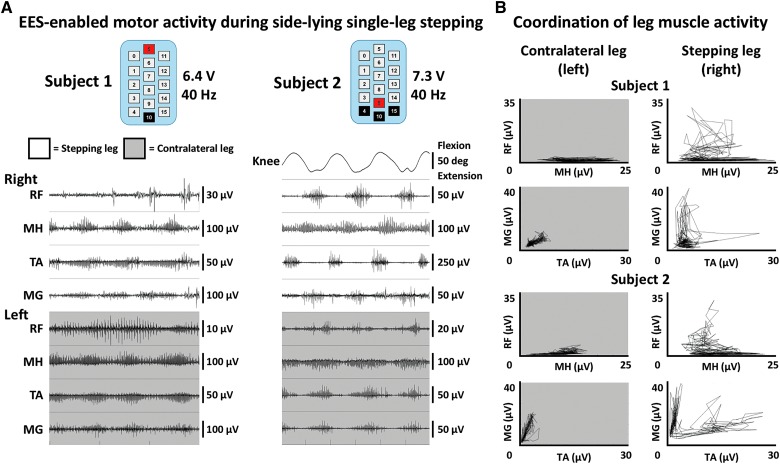
Epidural electrical stimulation (EES) of the spinal cord has been shown to restore function after spinal cord injury (SCI). Characterization of EES-evoked motor responses has provided a basic understanding of spinal sensorimotor network activity related to EES-enabled motor activity of the lower extremities. However, the use of EES-evoked motor responses to guide EES system implantation over the spinal cord and their relation to post-operative EES-enabled function in humans with chronic paralysis attributed to SCI has yet to be described. Herein, we describe the surgical and intraoperative electrophysiological approach used, followed by initial EES-enabled results observed in 2 human subjects with motor complete paralysis who were enrolled in a clinical trial investigating the use of EES to enable motor functions after SCI. The 16-contact electrode array was initially positioned under fluoroscopic guidance. Then, EES-evoked motor responses were recorded from select leg muscles and displayed in real time to determine electrode array proximity to spinal cord regions associated with motor activity of the lower extremities. Acceptable array positioning was determined based on achievement of selective proximal or distal leg muscle activity, as well as bilateral muscle activation. Motor response latencies were not significantly different between intraoperative recordings and post-operative recordings, indicating that array positioning remained stable. Additionally, EES enabled intentional control of step-like activity in both subjects within the first 5 days of testing. These results suggest that the use of EES-evoked motor responses may guide intraoperative positioning of epidural electrodes to target spinal cord circuitry to enable motor functions after SCI.
Keywords: electrically evoked spinal motor potentials; epidural electrical stimulation, spinal cord injury; neuromodulation; spinal cord intraoperative electrophysiology.
Conflict of interest statement
V.R.E. and Y.P.G. are shareholders in NeuroRecovery Technologies. V.R.E. is president and chair of the company's board of directors. V.R.E. and Y.P.G. hold investorship rights on intellectual property licensed by the regents of the University of California to NeuroRecovery Technologies and its subsidiaries.
Figures
References
-
- Harvey L.A. (2016). Physiotherapy rehabilitation for people with spinal cord injuries. J. Physiother. 62, 4–11 - PubMed
-
- Sekhon L.H., and Fehlings M.G. (2001). Epidemiology, demographics, and pathophysiology of acute spinal cord injury. Spine (Phila Pa 1976) 26, 24 Suppl., S2–S12 - PubMed
-
- Bydon M., Lin J., Macki M., Gokaslan Z.L., and Bydon A. (2014). The current role of steroids in acute spinal cord injury. World Neurosurg. 82, 848–854 - PubMed
-
- Chen B.K., Madigan N.N., Hakim J.S., Dadsetan M., McMahon S.S., Yaszemski M.J., and Windebank A.J. (2018). GDNF Schwann cells in hydrogel scaffolds promote regional axon regeneration, remyelination and functional improvement after spinal cord transection in rats. J. Tissue Eng. Regen. Med. 12, e398–e407 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical