

Review
doi: 10.1513/AnnalsATS.201806-380AW.
Host and Viral Determinants of Respiratory Syncytial Virus-induced Airway Mucus
Affiliations
- PMID: 30431348
- PMCID: PMC6322028
- DOI: 10.1513/AnnalsATS.201806-380AW
Item in Clipboard
Review
Host and Viral Determinants of Respiratory Syncytial Virus-induced Airway Mucus
Ann Am Thorac Soc.
2018 Nov.
Abstract
Respiratory syncytial virus (RSV) is a leading cause of hospitalization of infants worldwide each year. Both host and viral factors host factors predispose a subset of what appear to be healthy infants to severe RSV-induced disease. In this review, we outline many genetic and immunologic factors that contribute to airway obstruction that contributes to the severity of RSV infection.
Keywords: IL-13; RSV; interferon; mucus.
Figures

Bronchiolar localization of respiratory syncytial virus (RSV) antigen. (A) Medium-sized muscular bronchioles demonstrate RSV antigen circumferentially and limited to surface epithelium (staining for RSV antigen using a polyclonal biotin-conjugated goat anti-RSV). Magnification ×25. (B) Bronchiolar epithelium demonstrating RSV antigen in surface epithelium. Basal epithelium is antigen negative, and ciliated (arrow) cells are clearly infected. It is likely that nonciliated cells are also infected because of the near-circumferential staining pattern (staining for RSV antigen using a polyclonal biotin-conjugated goat anti-RSV). Intraluminal debris in small airways, including epithelium and inflammatory cells, stains positive for RSV antigen. Magnification ×250. (C) Histopathological features of bronchiolar inflammation. Acute bronchiolitis is shown in medium-sized airway with intraluminal cell fragments composed of dead epithelium and inflammatory cells, as well as amorphous debris, in 1931 case (hematoxylin and eosin stain). Magnification ×62.5. (D) Intraluminal debris includes mucus, fibrin, epithelial cells, and inflammatory cells in 1949 case (periodic acid–Schiff stain). Magnification ×250. Reprinted by permission from Reference .

Respiratory syncytial virus (RSV) infects airway epithelial cells, eliciting the production of type I (α and β) and type III (λ) interferons (IFNs), which bind to the type I interferon receptor (IFNAR) to stimulate natural killer (NK), NKT, CD4, and CD8 cell production of type II (γ) IFN.

Respiratory syncytial virus (RSV) infects airway epithelial cells, inducing the expression of thymic stromal lymphopoietin (TSLP) that binds to the thymic stromal lymphopoietin receptor (TSLPR) on type 2 innate lymphoid cells (ILC2), resulting in ILC2 expansion and production of interleukin (IL)-13. IL-13 produced by ILC2 cells induces epithelial cell mucous metaplasia that contributes to airway hyperresponsiveness (AHR). Th2 = T-helper cell type 2 cells.

Infection of BALB/c mice with respiratory syncytial virus (RSV) strain 01/2-20 induced airway mucin expression and luminal mucus accumulation that was partially dependent on thymic stromal lymphopoietin (TSLP) signaling. Representative periodic acid–Schiff–stained sections of mucus-containing airways in the lungs on Day 6 after infection. The arrowhead denotes intraluminal mucus plugging. TSLPR KO = thymic stromal lymphopoietin receptor knockout. Scale bar = 200 μm. Reprinted by permission from Reference .
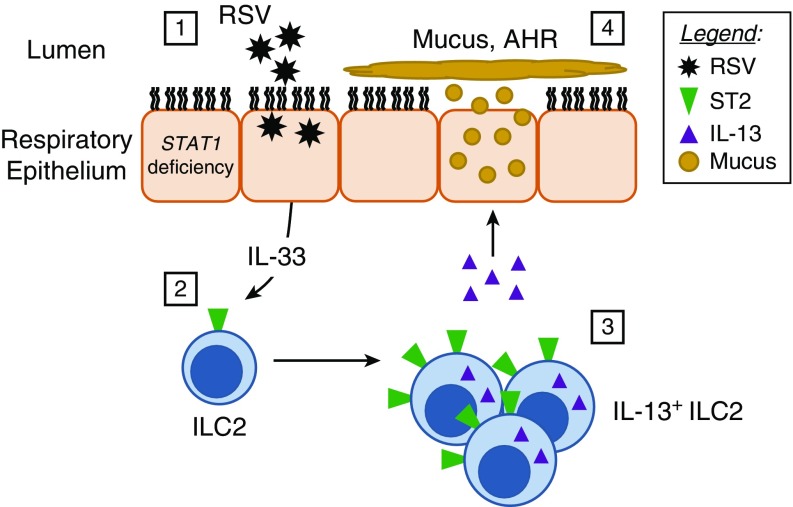
Respiratory syncytial virus (RSV) infection of airway epithelial cells in the setting of STAT1 (signal transducer and activator of transcription 1) deficiency increases epithelial cell interleukin (IL)-33 expression, activating type 2 innate lymphoid cells (ILC2) to produce IL-13, resulting in mucous metaplasia and airway hyperresponsiveness (AHR).

Respiratory syncytial virus (RSV) strain A2 infection induced Gob5 expression in STAT1−/− (signal transducer and activator of transcription 1–deficient) mice. Representative sections of medium-sized bronchi (Day 14 after infection) stained with anti-Gob5 antibody. Magnification ×200. Reprinted by permission from Reference . KO = knockout; WT = wild type.
References
-
- Fryzek JP, Martone WJ, Groothuis JR. Trends in chronologic age and infant respiratory syncytial virus hospitalization: an 8-year cohort study. Adv Ther. 2011;28:195–201. - PubMed
-
- Leader S, Kohlhase K. Respiratory syncytial virus-coded pediatric hospitalizations, 1997 to 1999. Pediatr Infect Dis J. 2002;21:629–632. - PubMed
-
- Leader S, Kohlhase K. Recent trends in severe respiratory syncytial virus (RSV) among US infants, 1997 to 2000. J Pediatr. 2003;143(5) Suppl:S127–S132. - PubMed
-
- Glick AF, Kjelleren S, Hofstetter AM, Subramony A. RSV hospitalizations in comparison with regional RSV activity and inpatient palivizumab administration, 2010–2013. Hosp Pediatr. 2017;7:271–278. - PubMed
-
- Berger TM, Aebi C, Duppenthaler A, Stocker M Swiss Pediatric Surveillance Unit. Prospective population-based study of RSV-related intermediate care and intensive care unit admissions in Switzerland over a 4-year period (2001–2005) Infection. 2009;37:109–116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
