

Comment
doi: 10.1513/AnnalsATS.201810-693CME.
Summary for Clinicians: Diagnosis of Primary Ciliary Dyskinesia
Affiliations
- PMID: 30433820
- PMCID: PMC7336768
- DOI: 10.1513/AnnalsATS.201810-693CME
Item in Clipboard
Comment
Summary for Clinicians: Diagnosis of Primary Ciliary Dyskinesia
Ann Am Thorac Soc.
2019 Feb.
No abstract available
Keywords: Kartagener syndrome; nitric oxide; primary ciliary dyskinesia; situs inversus.
Figures
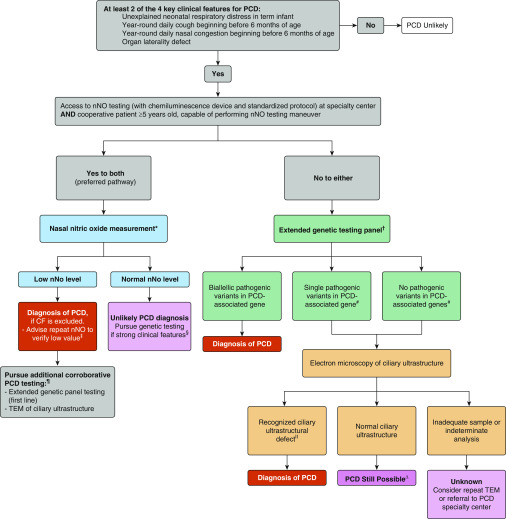
Suggested diagnostic algorithm for evaluating the patient with suspected primary ciliary dyskinesia (PCD). *Cystic fibrosis (CF) should be ruled out before performing nasal nitric oxide (nNO) measurement, as roughly one-third of patients with CF can have nNO values below PCD diagnostic cutoffs. nNO measurements should only be performed with chemiluminescence analyzers using standardized protocols at centers with specific expertise in nNO measurements. Some nNO analyzers have not received approval from federal agencies worldwide (U.S. Food and Drug Administration and Health Canada have not approved all chemiluminescence devices for clinical use), which may have implications for clinical implementation. †Genetic panels testing for mutations in more than 12 disease-associated PCD genes, including deletion/duplication analysis. ‡As nNO levels can be significantly decreased by viral respiratory tract infections, a repeat nNO measurement, at least 2 weeks after the initial low value (expert opinion), is recommended to ensure that the initial low value is not secondary to a viral process. A normal nNO value on repeat testing suggests that the patient does not have PCD, as nNO values remain consistently low in PCD. §Most forms of PCD resulting in normal nNO levels have normal or nondiagnostic electron microscopy studies. Thus, genetic testing is recommended in these cases. #Variants of unknown significance also require further work-up. For the purposes of the algorithm, “likely pathogenic” variants and “pathogenic” variants or grouped together as pathogenic. ¶Additional corroborative testing may provide information on clinical prognosis and further understanding of the disease and suggest potential future therapeutic consideration. ǁKnown disease-associated transmission electron microscopy ultrastructural defects include outer dynein arm plus inner dynein arm (IDA) defects, IDA defects with microtubular disorganization, and absent central pair, identified using established criteria (1, 6, 13). Of note, the presence of IDA defects alone is rarely diagnostic for PCD .∆Up to 30% of PCD cases can have normal ciliary ultrastructure of electron microscopy (EM). Consider referral to PCD specialty center if there is a strong clinical phenotype but all EM and genetic testing are negative. TEM = transmission electron microscopy. Reprinted by permission from Reference .
Comment on
-
Diagnosis of Primary Ciliary Dyskinesia. An Official American Thoracic Society Clinical Practice Guideline.Am J Respir Crit Care Med. 2018 Jun 15;197(12):e24-e39. doi: 10.1164/rccm.201805-0819ST. Am J Respir Crit Care Med. 2018. PMID: 29905515 Free PMC article.
References
-
- Simoneau T, Zandieh SO, Rao DR, Vo P, Palm KE, McCown M, et al. Impact of cilia ultrastructural examination on the diagnosis of primary ciliary dyskinesia. Pediatr Dev Pathol. 2013;16:321–326. - PubMed
-
- Shoemark A, Dixon M, Corrin B, Dewar A. Twenty-year review of quantitative transmission electron microscopy for the diagnosis of primary ciliary dyskinesia. J Clin Pathol. 2012;65:267–271. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
