

A Bayesian network meta-analysis on the efficacy and safety of eighteen targeted drugs or drug combinations for pulmonary arterial hypertension
- PMID: 30442035
- PMCID: PMC6249551
- DOI: 10.1080/10717544.2018.1523257
A Bayesian network meta-analysis on the efficacy and safety of eighteen targeted drugs or drug combinations for pulmonary arterial hypertension
Abstract
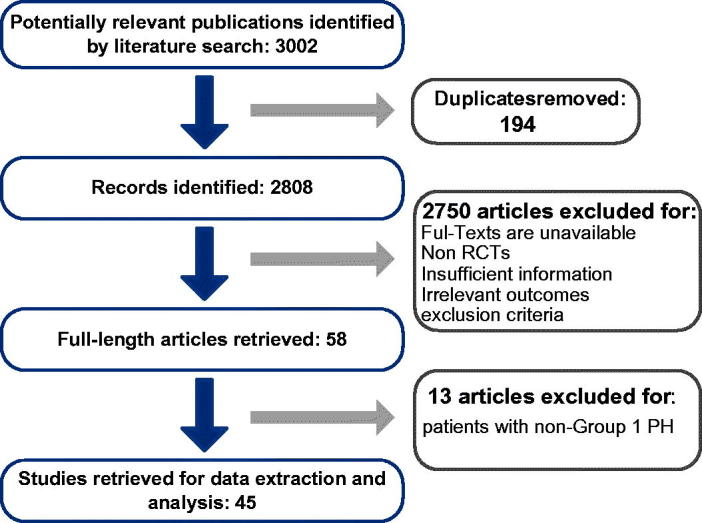
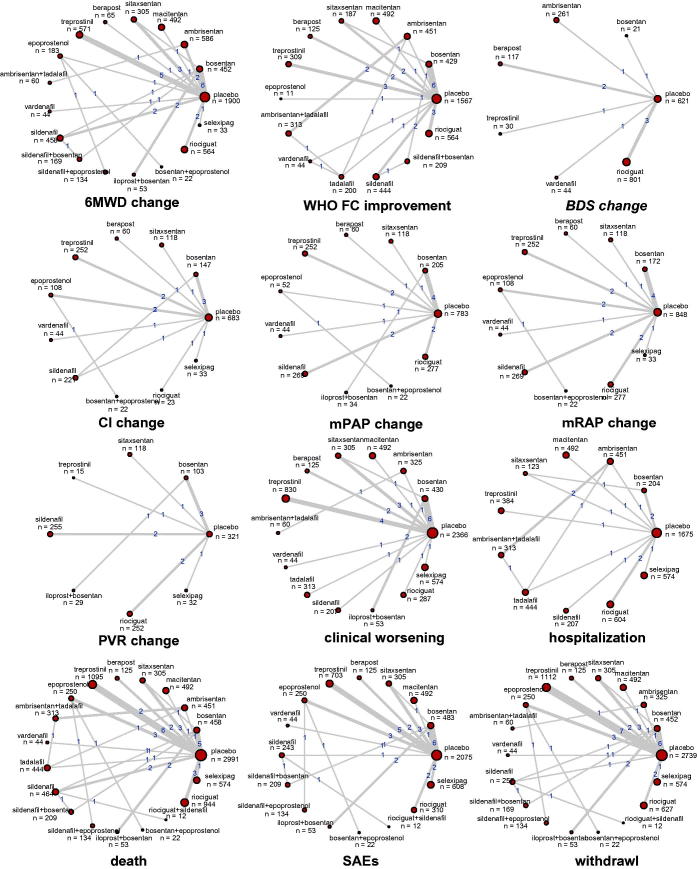
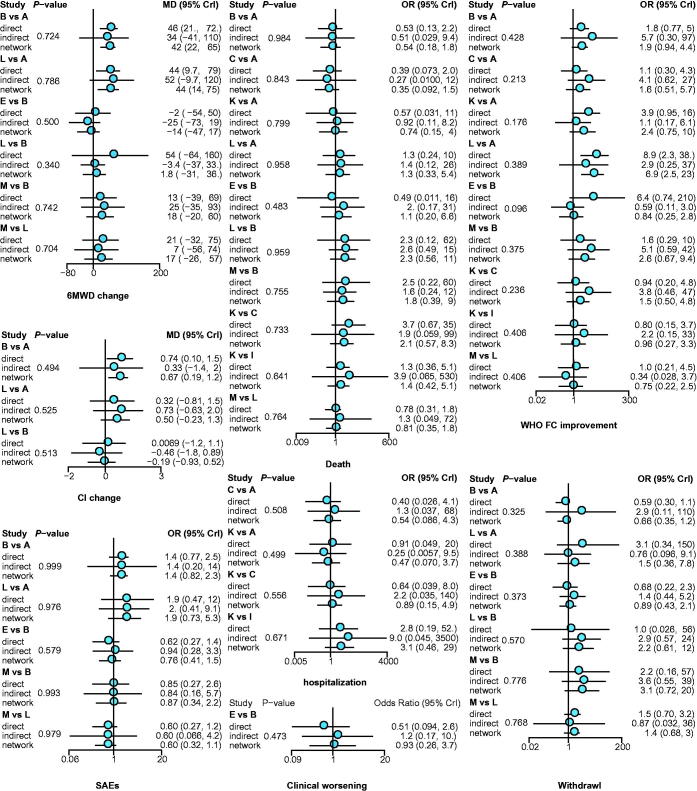
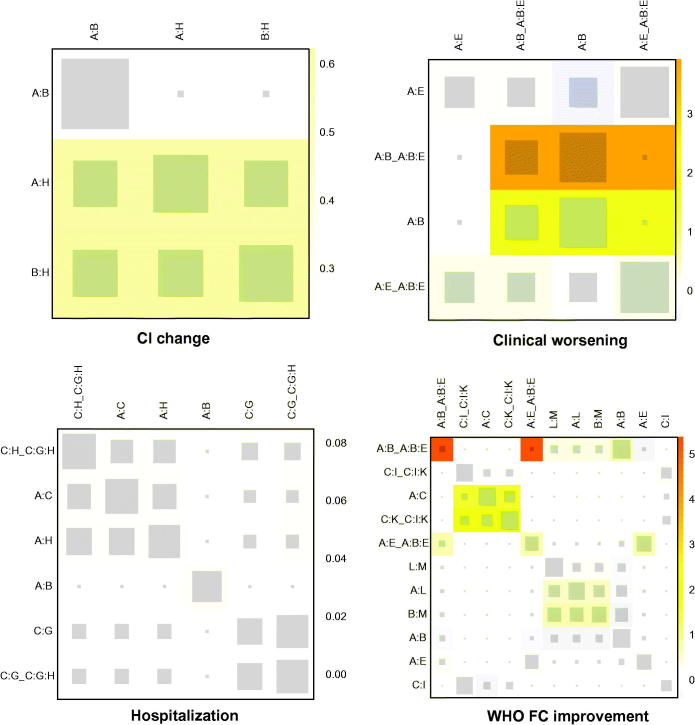
Pulmonary arterial hypertension (PAH) can be relieved by pharmacological interventions, especially the targeted drug, which is classified into endothelin receptor antagonist, phosphodiesterase 5 inhibitor, prostaglandin I2, soluble guanylate cyclase stimulator and selective non-prostanoid prostacyclin receptor agonist. To solve the contradictions existing in reported trials and provide a comprehensive guideline for clinical practice. PubMed, Embase, Cochrane library, and clinicaltrials.gov were searched. The basic information about the article, trial, arm, intervention, and the detailed data of outcome, including 6 minutes walking distance (6MWD) change, WHO functional class (FC) improvement, Borg dyspnea score (BDS) change, cardiac index (CI) change, mean pulmonary arterial pressure (mPAP) change, mean right arterial pressure (mRAP) change, pulmonary vascular resistance (PVR) change, clinical worsening, hospitalization, death, severe adverse events (SAEs), and withdrawal were extracted. The rank of treatments was estimated. 10,230 cases provided the firsthand comparison data about targeted drugs for treating PAH. For 6MWD, ambrisentan + tadalafil, vardenafil, and sildenafil + bosentan were better than others. Epoprostenol, macitentan, and sildenafil represented a greater WHO FC improvement. Vardenafil and treprostinil were better for BDS. So were bosentan + epoprostenol and bosentan alone for CI. Iloprost plus bosentan, bosentan + epoprostenol, and epoprostenol were better for mPAP. Iloprost plus bosentan, bosentan alone, and selexipag could reduce PVR. Sildenafil, epoprostenol, and vardenafil had the highest probability to reduce the incidence of death and withdrawal. To conclude, vardenafil and iloprost + bosentan showed relatively better performance in both efficacy and safety. However, the therapeutic choice should be made according to both the feature of each therapy and the individual condition.
Keywords: 6 minutes walking distance; Pulmonary arterial hypertension; functional class; network meta-analysis; randomized controlled trial.
Figures
References
-
- Aessopos A, Stamatelos G, Skoumas V, et al. (1995). Pulmonary hypertension and right heart failure in patients with beta-thalassemia intermedia. Chest 107:50–3. - PubMed
-
- Badesch DB, Bodin F, Channick RN, et al. (2002). Complete results of the first randomized, placebo-controlled study of bosentan, a dual endothelin receptor antagonist, in pulmonary arterial hypertension. Curr Ther Res 63:227–46.
-
- Badesch DB, Hill NS, Burgess G, et al. (2007). Sildenafil for pulmonary arterial hypertension associated with connective tissue disease. J Rheumatol 34:2417–22. - PubMed
-
- Badesch DB. (2000). Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann Intern Med 132:425–34. - PubMed
-
- Barst RJ, et al. (2006). Treatment of pulmonary arterial hypertension with the selective endothelin-A receptor antagonist sitaxsentan. J Am Coll Cardiol 47:2049–56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials