

Environmental factors and risk of delirium in geriatric patients: an observational study
- PMID: 30442109
- PMCID: PMC6238358
- DOI: 10.1186/s12877-018-0977-y
Environmental factors and risk of delirium in geriatric patients: an observational study
Abstract
Background: Patients with delirium have increased risk of death, dementia and institutionalization, and prognosis differs between delirium motor subtypes. A few studies have identified associations between environmental factors like room-transfers and time spent in the emergency department (ED) and delirium, but no studies have investigated if environmental factors may influence delirium motor subtypes. We wanted to explore if potentially stressful events like ward-transfers, arriving ED at nighttime, time spent in ED and nigthttime investigations were associated with development of delirium (incident delirium) and delirium motor subtypes.
Methods: We used the DSM-5 criteria to diagnose delirium and the Delirium Motor Subtype Scale for motor subtyping. We defined hyperactive and mixed delirium as delirium with hyperactive symptoms, and hypoactive and no-subtype delirium as delirium without hyperactive symptoms. We registered ward-transfers, time of arrival in ED, time spent in ED and nighttime investigations (8 p.m. to 8 a.m.), and calculated Global Deterioration Scale (GDS) and Cumulative Illness Rating Scale (CIRS) to adjust for cognitive impairment and comorbidity. We used logistic regression analyses with incident delirium and delirium with hyperactive symptoms as outcome variables, and ward-transfers, arriving ED at nighttime, time spent in ED and nighttime investigations as exposure variables, adjusting for age, GDS and CIRS in the analyses for incident delirium.
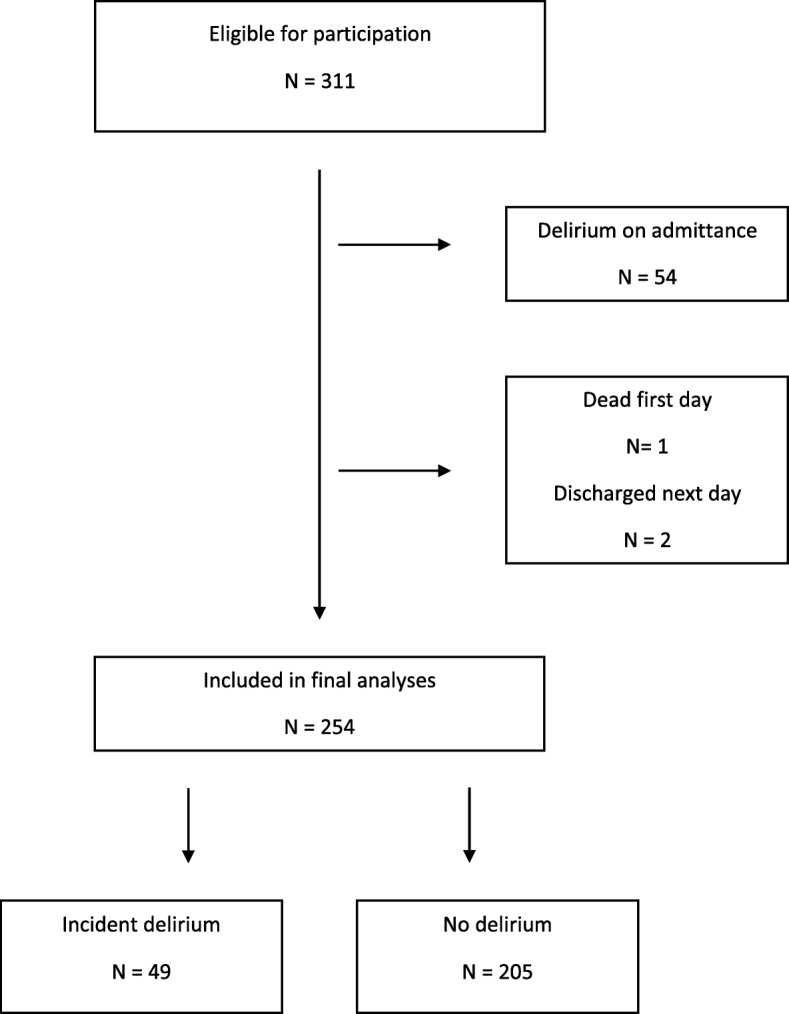
Results: We included 254 patients, mean age 86.1 years (SD 5.2), 49 (19.3%) had incident delirium, 22 with and 27 without hyperactive symptoms. There was a significant association between nighttime investigations and incident delirium in both the unadjusted (odds ratio (OR) 2.22, 95% confidence interval (CI) 1.17 to 4.22, p = 0.015) and the multiadjusted model (OR 2.61, CI 1.26 to 5.40, p = 0.010). There were no associations between any other exposure variables and incident delirium. No exposure variables were associated with delirium motor subtypes.
Conclusions: Nighttime investigations were associated with incident delirium, even after adjusting for age, cognitive impairment and comorbidity. We cannot out rule that the medical condition leading to nighttime investigations is the true delirium-trigger, so geriatric patients must still receive emergency investigations at nighttime. Hospital environment in broad sense may be a target for delirium prevention.
Keywords: Delirium; Environmental; Geriatric patients; Hospital; Risk factors.
Conflict of interest statement
Ethics approval and consent to participate
We confirm that all patients or a proxy consented for participation based on the concept of written informed consent. The Regional Committee for Medical and Health Research Ethics of Mid-Norway approved the study (REK Central 2015/474).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
