

Mucopolysaccharidoses: early diagnostic signs in infants and children
- PMID: 30442162
- PMCID: PMC6238260
- DOI: 10.1186/s13052-018-0550-5
Mucopolysaccharidoses: early diagnostic signs in infants and children
Abstract
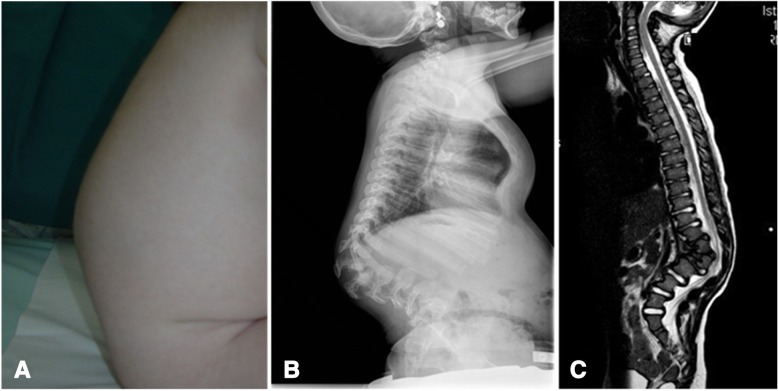
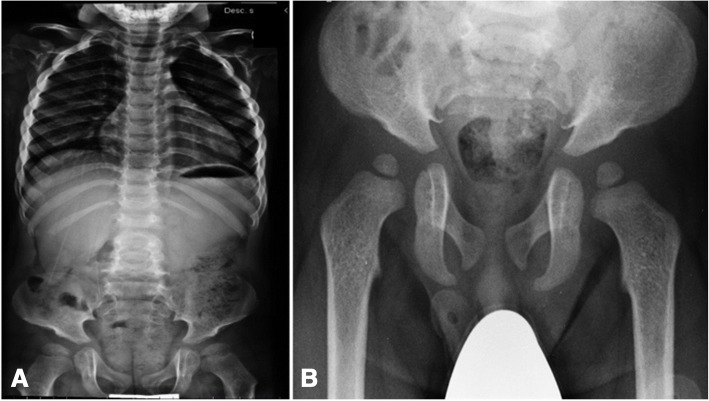
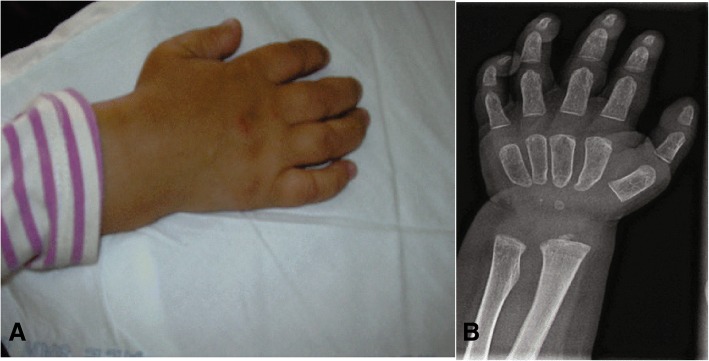
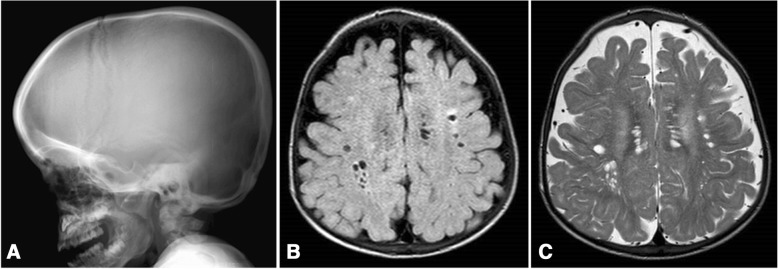
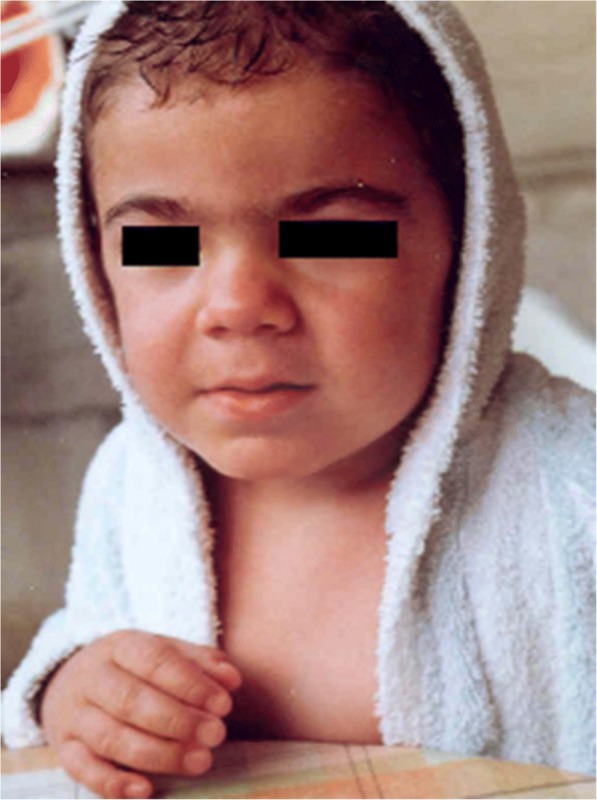
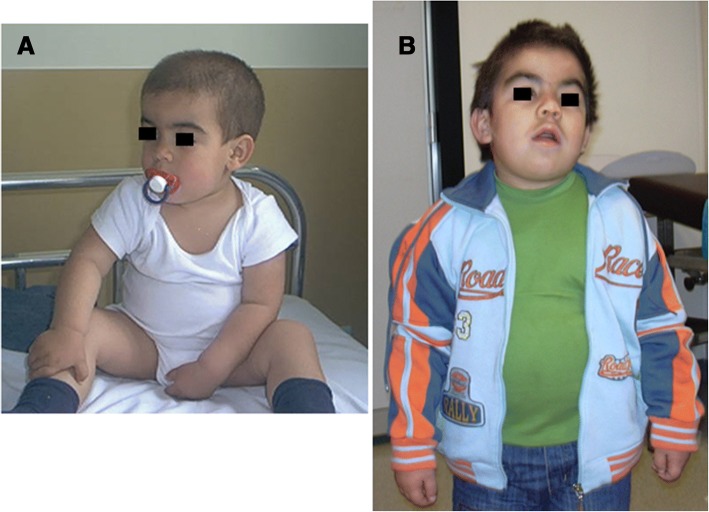
Mucopolysaccharidoses (MPS) comprise a group of lysosomal disorders that are characterized by progressive, systemic clinical manifestations and a coarse phenotype. The different types, having clinical, biochemical, and genetic heterogeneity, share key clinical features in varying combinations, including joint and skeletal dysplasia, coarse facial features, corneal clouding, inguinal or abdominal hernias, recurrent upper respiratory tract infections, heart valve disease, carpal tunnel syndrome, and variable neurological involvement. In the severe forms, these features usually appear in the first months of life, but a correct diagnosis is often reached later when suggestive signs are manifest. All MPS types may have severe or attenuated presentations depending on the residual enzymatic activity of the patient. Based on data from the literature and from personal experience, here we underline the very early signs of the severe forms which should alert the paediatrician on their first appearance. A few early signs are typical of MPS (i.e. gibbus) while many are unspecific (hernias, upper airway infections, organomegaly, etc.), and finding the association of many unspecific signs might prompt the paediatrician to search for a common cause and to carefully look for other more specific signs (gibbus and other skeletal deformities, heart murmur). We stress the need to increase awareness of MPS among paediatricians and other specialists to shorten the still existing diagnostic delay. A timely diagnosis is mandatory for the commencement of treatment as soon as possible, when available, to possibly obtain better results.
Keywords: Early MPS signs; Early MPS symptoms; Early-onset MPS; MPS; Mucopolysaccharidosis.
Conflict of interest statement
Consent for publication
The patients or their parents/guardians gave written consent for publication of their pictures.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Wraith JE, Jones S. Mucopolysaccharidosis type I. Pediatr Endrocrinol Rev. 2014;12(Suppl 1):102–106. - PubMed
-
- Bertola F, Filocamo M, Casati G, Mort M, Rosano C, Tylki-Szymanska A, et al. IDUA mutational profiling of a cohort of 102 European patients with mucopolysaccharidosis type I: identification and characterization of 35 novel α-L-iduronidase (IDUA) alleles. Hum Mutat. 2011;32(6):E2189–E2210. doi: 10.1002/humu.21479. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
