

Evaluating the urban-rural paradox: The complicated relationship between distance and the receipt of guideline-concordant care among cervical cancer patients
- PMID: 30442384
- PMCID: PMC6321781
- DOI: 10.1016/j.ygyno.2018.11.010
Evaluating the urban-rural paradox: The complicated relationship between distance and the receipt of guideline-concordant care among cervical cancer patients
Abstract
Objective: Urban-rural health disparities are often attributed to the longer distances rural patients travel to receive care. However, a recent study suggests that distance to care may affect urban and rural cancer patients differentially. We examined whether this urban-rural paradox exists among patients with cervical cancer.
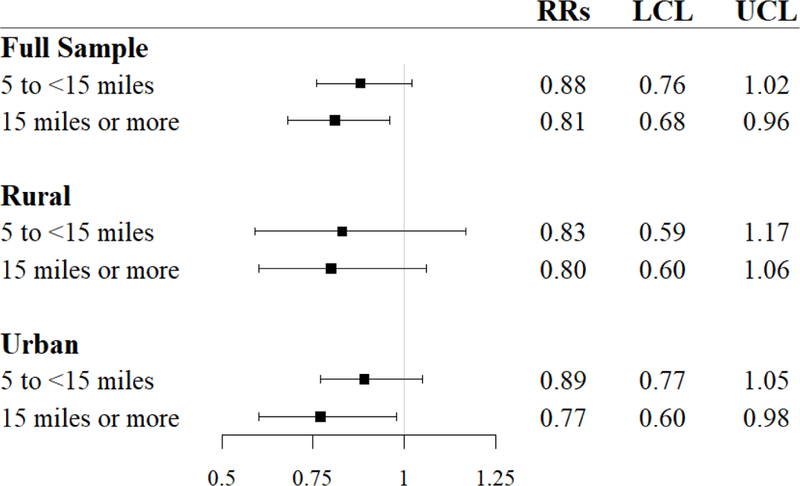
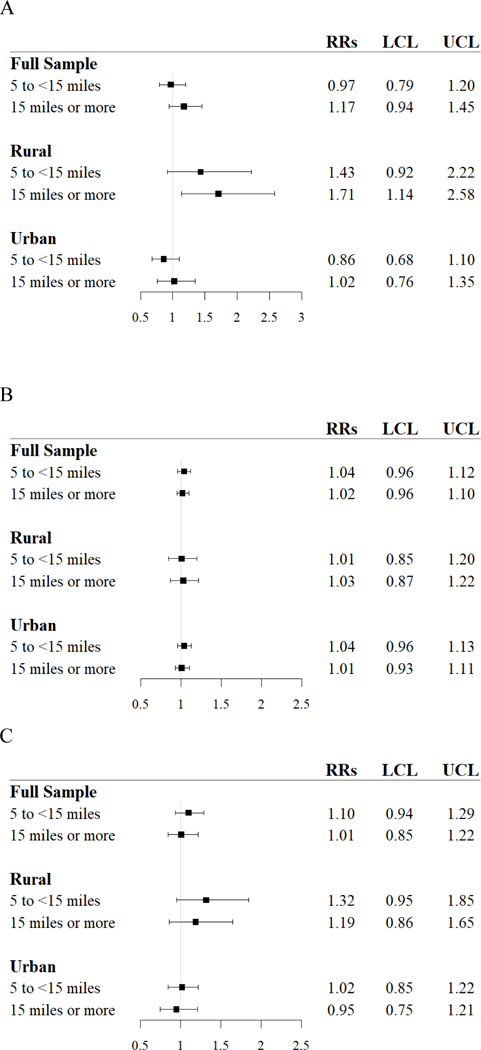
Methods: We identified individuals diagnosed with cervical cancer from 2004 to 2013 using a statewide cancer registry linked to multi-payer, insurance claims. Our primary outcome was receipt of guideline-concordant care: surgery for stages IA1-IB1; external beam radiation therapy (EBRT), concomitant chemotherapy, and brachytherapy for stages IB2-IVA. We estimated risk ratios (RR) using modified Poisson regressions, stratified by urban/rural location, to examine the association between distance to nearest facility and receipt of treatment.
Results: 62% of 999 cervical cancer patients received guideline-concordant care. The association between distance and receipt of care differed by type of treatment. In urban areas, cancer patients who lived ≥15 miles from the nearest surgical facility were less likely to receive primary surgical management compared to those <5 miles from the nearest surgical facility (RR: 0.77, 95% CI: 0.60-0.98). In rural areas, patients living ≥15 miles from the nearest brachytherapy facility were more likely to receive treatment compared to those <5 miles from the nearest brachytherapy facility (RR: 1.71, 95% CI: 1.14-2.58). Distance was not associated with the receipt of chemotherapy or EBRT.
Conclusions: Among cervical cancer patients, there is evidence supporting the urban-rural paradox, i.e., geographic distance to cancer care facilities is not consistently associated with treatment receipt in expected or consistent ways. Healthcare systems must consider the diverse and differential barriers encountered by urban and rural residents to improve access to high quality cancer care.
Keywords: Cervical cancer patients; Disparities; Distance to care; Guideline-concordant care; Urban/rural.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Figures
References
-
- Mayadev J, Klapheke A, Yashar C, et al. Underutilization of brachytherapy and disparities in survival for patients with cervical cancer in California. Gynecol Oncol (in press) - PubMed
-
- Rauh-Hain JA, Melamed A, Schaps D, et al. Racial and ethnic disparities over time in the treatment and mortality of women with gynecological malignancies. Gynecol Oncol 2018;149:4–11. - PubMed
-
- Singh GK, Miller BA, Hankey BF, et al. Persistent area socioeconomic disparities in US incidence of cervical cancer, mortality, stage, and survival, 1975–2000. Cancer 2004;101:1051–1057. - PubMed
