

Targeting B-cell maturation antigen with GSK2857916 antibody-drug conjugate in relapsed or refractory multiple myeloma (BMA117159): a dose escalation and expansion phase 1 trial
- PMID: 30442502
- PMCID: PMC6328058
- DOI: 10.1016/S1470-2045(18)30576-X
Targeting B-cell maturation antigen with GSK2857916 antibody-drug conjugate in relapsed or refractory multiple myeloma (BMA117159): a dose escalation and expansion phase 1 trial
Abstract
Background: B-cell maturation antigen (BCMA) is a cell-surface receptor of the tumour necrosis superfamily required for plasma cell survival. BMCA is universally detected on patient-derived myeloma cells and has emerged as a selective antigen to be targeted by novel treatments in multiple myeloma. We assessed the safety, tolerability, and preliminary clinical activity of GSK2857916, a novel anti-BCMA antibody conjugated to microtubule-disrupting agent monomethyl auristatin F, in patients with relapsed and refractory multiple myeloma.
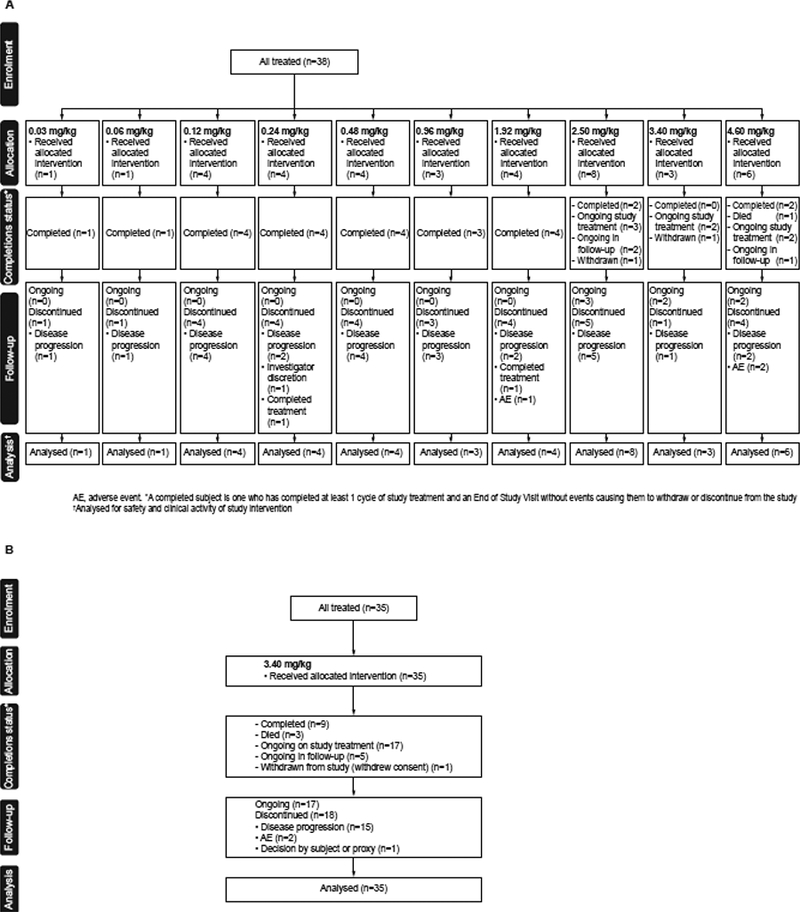
Methods: We did an international, multicentre, open-label, first-in-human phase 1 study with dose escalation (part 1) and dose expansion (part 2) phases, at nine centres in the USA, Canada, and the UK. Adults with histologically or cytologically confirmed multiple myeloma, Eastern Cooperative Oncology Group performance status 0 or 1, and progressive disease after stem cell transplantation, alkylators, proteasome inhibitors, and immunomodulators were recruited for this study. In part 1, patients received GSK2857916 (0·03-4·60 mg/kg) through 1 h intravenous infusions once every 3 weeks. In part 2, patients received the selected recommended phase 2 dose of GSK2857916 (3·40 mg/kg) once every 3 weeks. Primary endpoints were maximum tolerated dose and recommended phase 2 dose. Secondary endpoints for part 2 included preliminary anti-cancer clinical activity. All patients who received one or more doses were included in this prespecified administrative interim analysis (data cutoff date June 26, 2017), which was done for internal purposes. This study is registered with ClinicalTrials.gov, number NCT02064387, and is ongoing, but closed for recruitment.
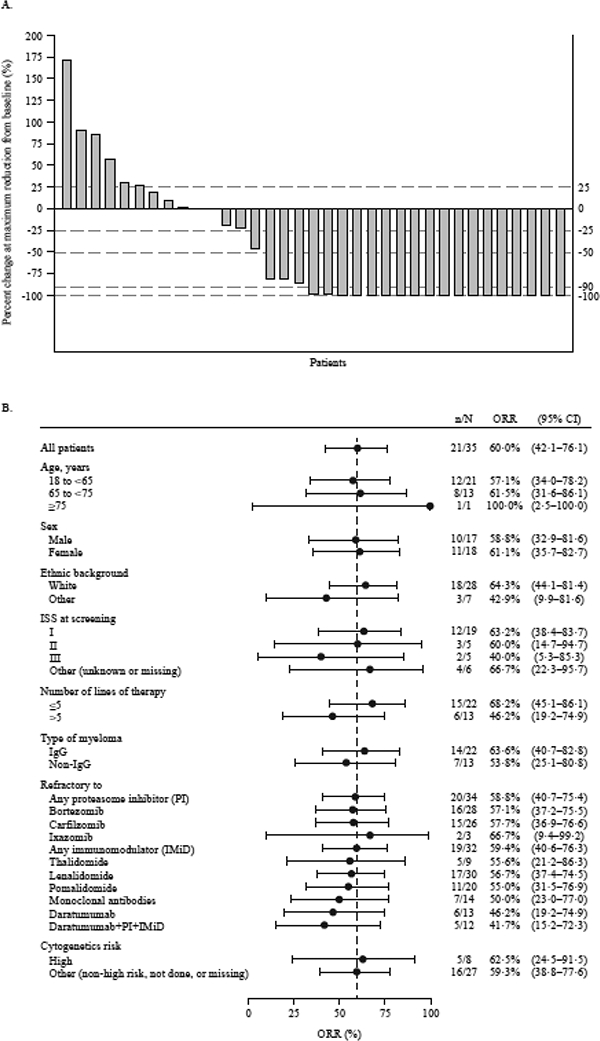
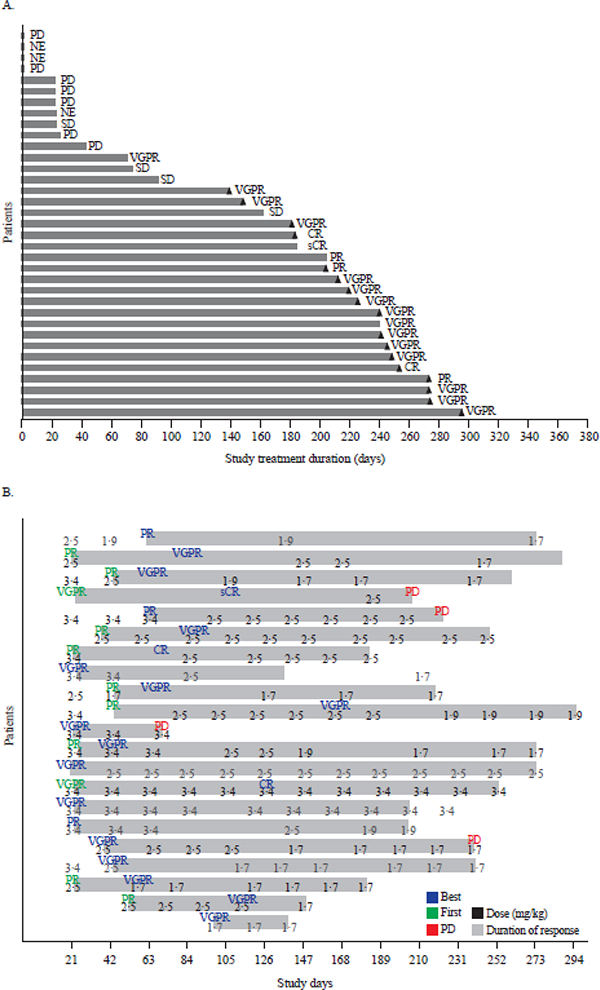
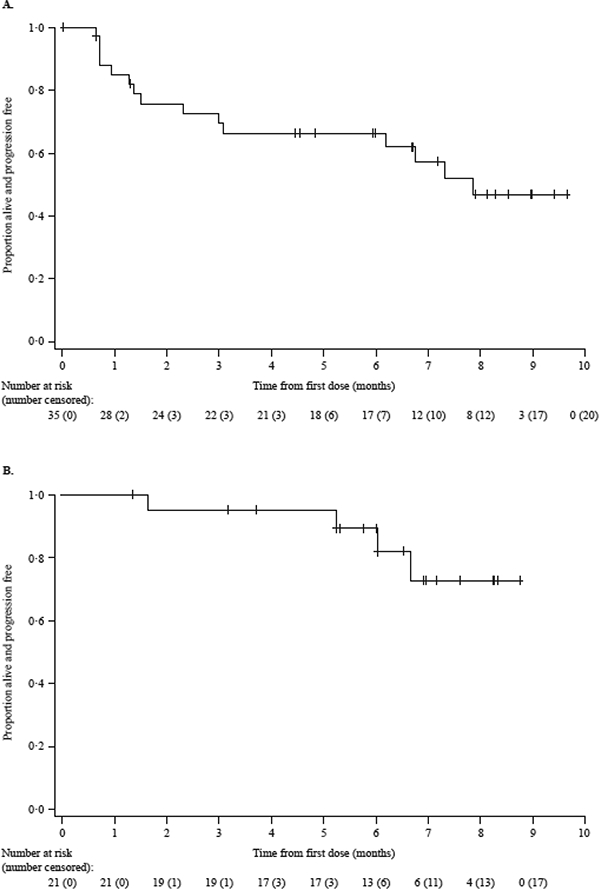
Findings: Between July 29, 2014, and Feb 21, 2017, we treated 73 patients: 38 patients in the dose-escalation part 1 and 35 patients in the dose-expansion part 2. There were no dose-limiting toxicities and no maximum tolerated dose was identified in part 1. On the basis of safety and clinical activity, we selected 3·40 mg/kg as the recommended phase 2 dose. Corneal events were common (20 [53%] of 38 patients in part 1 and 22 [63%] of 35 in part 2); most (18 [47%] in part 1 and 19 [54%] in part 2) were grade 1 or 2 and resulted in two treatment discontinuations in part 1 and no discontinuations in part 2. The most common grade 3 or 4 events were thrombocytopenia (13 [34%] of 38 patients in part 1 and 12 [34%] of 35 in part 2) and anaemia (6 [16%] in part 1 and 5 [14%] in part 2). There were 12 treatment-related serious adverse events and no treatment-related deaths. In part 2, 21 (60·0%; 95% CI 42·1-76·1) of 35 patients achieved an overall response.
Interpretation: At the identified recommended phase 2 dose, GSK2857916 was well tolerated and had good clinical activity in heavily pretreated patients, thereby indicating that this might be a promising candidate for the treatment of relapsed or refractory multiple myeloma.
Funding: GlaxoSmithKline.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DECLARATIONS OF INTEREST
LDA has participated in speakers’ bureaux for Celgene, Takeda and Amgen. ADC is a consultant for and a member of an advisory board for GlaxoSmithKline and Celgene, is a member of an advisory board for Janssen and Bristol-Myers Squibb, has received research funding from Bristol-Myers Squibb, Celgene and Novartis. AH is an employee of and holds stocks/shares in GlaxoSmithKline and is a non-executive director and holds stocks in Imugene. NL has received research funding from GlaxoSmithKline; RP has received honoraria from Janssen, Takeda, Celgene, and Amgen, and travel support to attend meetings from Janssen, Takeda, and Celgene. PGR is a consultant for, and has received research funding from, Celgene, Takeda, and Jazz Pharmaceuticals, and is a member of the board of directors/advisory committee for Celgene, Jazz Pharmaceuticals, Janssen, and Millennium. HJS has received honoraria from Janssen, Celgene, and Amgen. ST is a consultant for and has received honoraria from Amgen and Celgene; has received honoraria from Takeda and AbbVie; is a consultant for Novartis; and has received research support from Janssen. PMV is a consultant for Amgen, Celgene, Janssen, Bristol-Myers Squibb, Novartis, Takeda, and Teneo-Bio, and has participated in speakers’ bureaux for Amgen, Celgene, and Janssen. KY is a consultant for Autolus, has received honoraria from Autolus, Amgen, Janssen, and Celgene, and has received research funding from Amgen, Janssen, Celgene, and Chugai. DJA, JBO, MMG, and ZH are employees of and hold stocks/shares in GlaxoSmithKline. SL was an employee of GlaxoSmithKline at the time of study conduct and holds stocks/shares in GlaxoSmithKline. BR and ENL declare no conflict of interest outside of the submitted work.
Figures
Comment in
-
Evolution of monoclonal antibodies in multiple myeloma.Lancet Oncol. 2018 Dec;19(12):1554-1555. doi: 10.1016/S1470-2045(18)30647-8. Epub 2018 Nov 12. Lancet Oncol. 2018. PMID: 30442500 No abstract available.
References
-
- Kumar SK, Dimopoulos MA, Kastritis E, et al. Natural history of relapsed myeloma, refractory to immunomodulatory drugs and proteasome inhibitors: a multicenter IMWG study. Leukemia 2017; 31(11): 2443–8. - PubMed
-
- Darce JR, Arendt BK, Wu X, Jelinek DF. Regulated expression of BAFF-binding receptors during human B cell differentiation. J Immunol 2007; 179(11): 7276–86. - PubMed
-
- Lee L, Bounds D, Paterson J, et al. Evaluation of B cell maturation antigen as a target for antibody drug conjugate mediated cytotoxicity in multiple myeloma. Br J Haematol 2016; 174(6): 911–22. - PubMed
-
- Sanchez E, Gillespie A, Tang G, et al. Soluble B-Cell Maturation Antigen Mediates Tumor-Induced Immune Deficiency in Multiple Myeloma. Clin Cancer Res 2016; 22(13): 3383–97. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
