

Feasibility, Acceptability, and Adoption of Digital Fingerprinting During Contact Investigation for Tuberculosis in Kampala, Uganda: A Parallel-Convergent Mixed-Methods Analysis
- PMID: 30442637
- PMCID: PMC6265600
- DOI: 10.2196/11541
Feasibility, Acceptability, and Adoption of Digital Fingerprinting During Contact Investigation for Tuberculosis in Kampala, Uganda: A Parallel-Convergent Mixed-Methods Analysis
Abstract
Background: In resource-constrained settings, challenges with unique patient identification may limit continuity of care, monitoring and evaluation, and data integrity. Biometrics offers an appealing but understudied potential solution.
Objective: The objective of this mixed-methods study was to understand the feasibility, acceptability, and adoption of digital fingerprinting for patient identification in a study of household tuberculosis contact investigation in Kampala, Uganda.
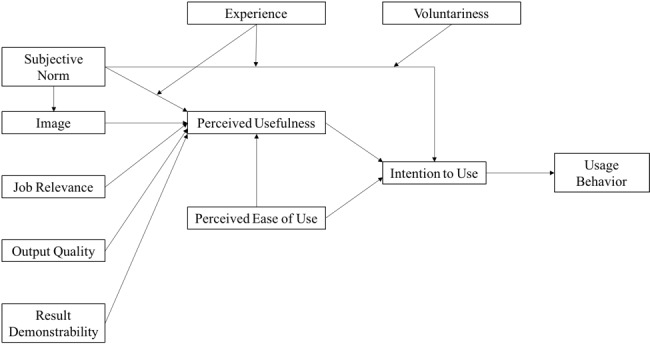
Methods: Digital fingerprinting was performed using multispectral fingerprint scanners. We tested associations between demographic, clinical, and temporal characteristics and failure to capture a digital fingerprint. We used generalized estimating equations and a robust covariance estimator to account for clustering. In addition, we evaluated the clustering of outcomes by household and community health workers (CHWs) by calculating intraclass correlation coefficients (ICCs). To understand the determinants of intended and actual use of fingerprinting technology, we conducted 15 in-depth interviews with CHWs and applied a widely used conceptual framework, the Technology Acceptance Model 2 (TAM2).
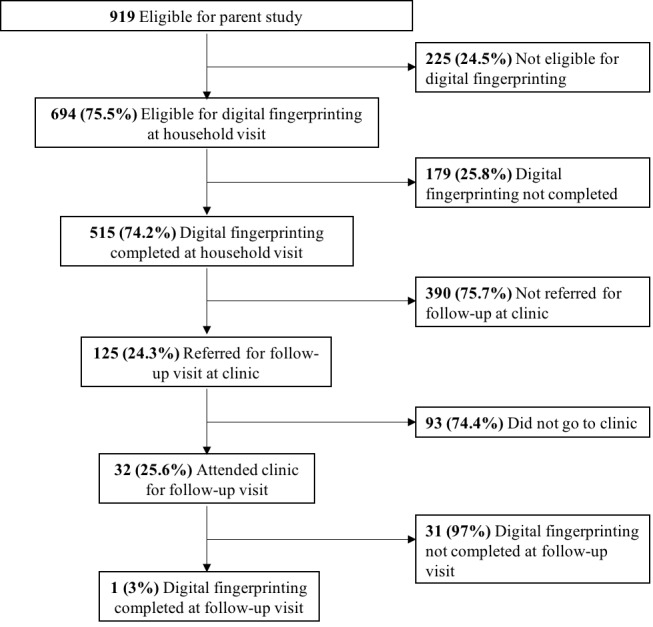
Results: Digital fingerprints were captured for 75.5% (694/919) of participants, with extensive clustering by household (ICC=.99) arising from software (108/179, 60.3%) and hardware (65/179, 36.3%) failures. Clinical and demographic characteristics were not markedly associated with fingerprint capture. CHWs successfully fingerprinted all contacts in 70.1% (213/304) of households, with modest clustering of outcomes by CHWs (ICC=.18). The proportion of households in which all members were successfully fingerprinted declined over time (ρ=.30, P<.001). In interviews, CHWs reported that fingerprinting failures lowered their perceptions of the quality of the technology, threatened their social image as competent health workers, and made the technology more difficult to use.
Conclusions: We found that digital fingerprinting was feasible and acceptable for individual identification, but problems implementing the hardware and software lead to a high failure rate. Although CHWs found fingerprinting to be acceptable in principle, their intention to use the technology was tempered by perceptions that it was inconsistent and of questionable value. TAM2 provided a valuable framework for understanding the motivations behind CHWs' intentions to use the technology. We emphasize the need for routine process evaluation of biometrics and other digital technologies in resource-constrained settings to assess implementation effectiveness and guide improvement of delivery.
Keywords: biometrics; mHealth; mobile phone; tuberculosis.
©Elizabeth B White, Amanda J Meyer, Joseph M Ggita, Diana Babirye, David Mark, Irene Ayakaka, Jessica E Haberer, Achilles Katamba, Mari Armstrong-Hough, John Lucian Davis. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 15.11.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Beck EJ, Shields JM, Tanna G, Henning G, de Vega I, Andrews G, Boucher P, Benting L, Garcia-Calleja JM, Cutler J, Ewing W, Kijsanayotin B, Kujinga T, Mahy M, Makofane K, Marsh K, Nacheeva C, Rangana N, Vega MFR, Sabin K, Varetska O, Macharia Wanyee S, Watiti S, Williams B, Zhao J, Nunez C, Ghys P, Low-Beer D. Developing and implementing national health identifiers in resource limited countries: why, what, who, when and how? Glob Health Action. 2018;11(1):1440782. doi: 10.1080/16549716.2018.1440782. http://europepmc.org/abstract/MED/29502484 - DOI - PMC - PubMed
-
- SonLa Study Group Using a fingerprint recognition system in a vaccine trial to avoid misclassification. Bulletin of the World Health Organization. 2007 Jan;85(1):64–67. http://www.scielosp.org/scielo.php?script=sci_arttext&pid=S0042-96862007... - PMC - PubMed
-
- Unar J, Seng WC, Abbasi A. A review of biometric technology along with trends and prospects. Pattern Recognition. 2014 Aug;47(8):2673–2688. doi: 10.1016/j.patcog.2014.01.016. - DOI
-
- Wall KM, Kilembe W, Inambao M, Chen YN, Mchoongo M, Kimaru L, Hammond YT, Sharkey T, Malama K, Fulton TR, Tran A, Halumamba H, Anderson S, Kishore N, Sarwar S, Finnegan T, Mark D, Allen SA. Implementation of an electronic fingerprint-linked data collection system: a feasibility and acceptability study among Zambian female sex workers. Global Health. 2015 Jun 27;11:27. doi: 10.1186/s12992-015-0114-z. https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992... - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
