

Impact of a Clinical Decision Support System on Guideline Adherence of Surveillance Recommendations for Colonoscopy After Polypectomy
- PMID: 30442733
- PMCID: PMC7210781
- DOI: 10.6004/jnccn.2018.7050
Impact of a Clinical Decision Support System on Guideline Adherence of Surveillance Recommendations for Colonoscopy After Polypectomy
Abstract
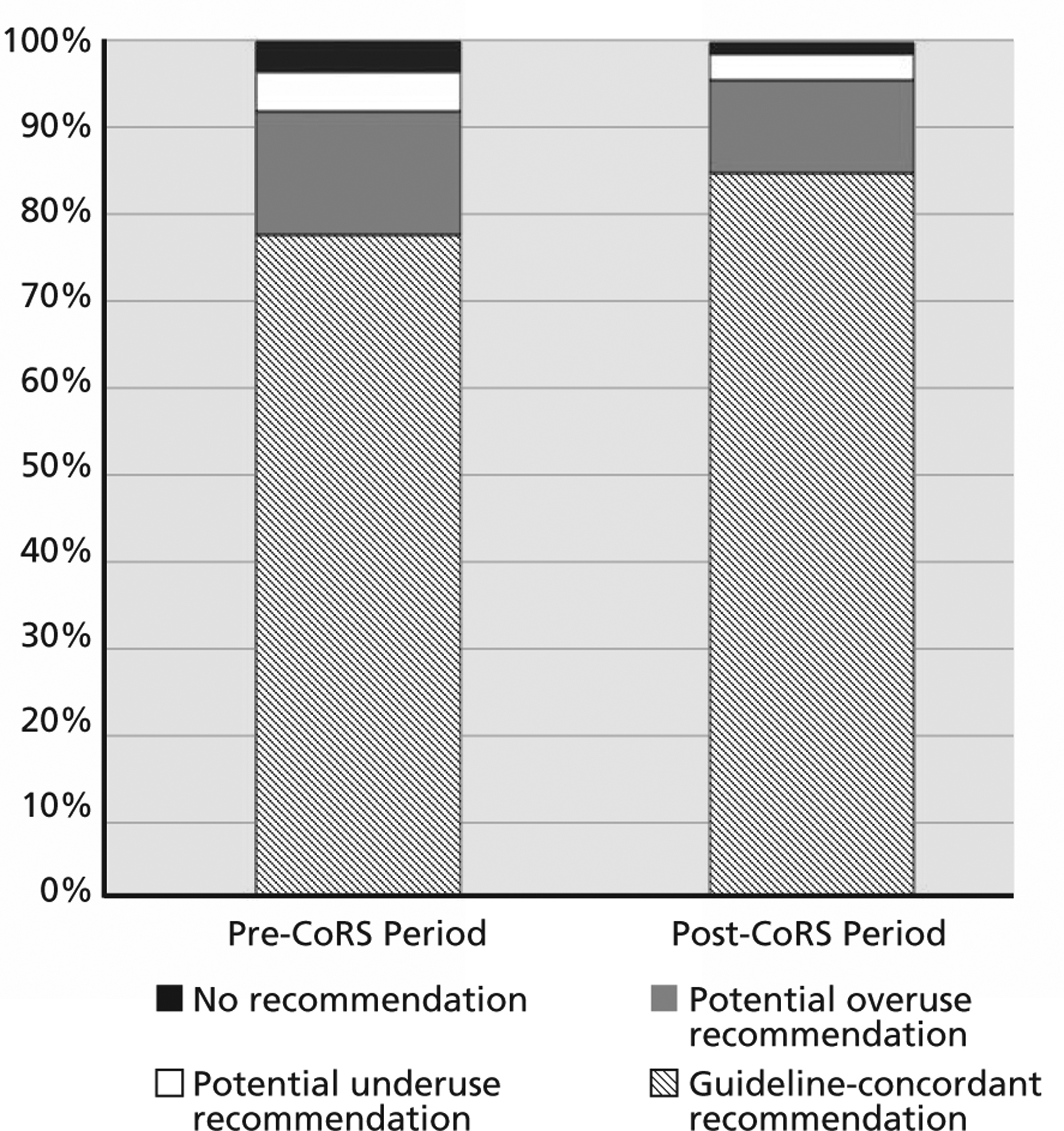
Background: Surveillance colonoscopy is required in patients with polyps due to an elevated colorectal cancer (CRC) risk; however, studies suggest substantial overuse and underuse of surveillance colonoscopy. The goal of this study was to characterize guideline adherence of surveillance recommendations after implementation of an electronic medical record (EMR)-based Colonoscopy Pathology Reporting and Clinical Decision Support System (CoRS). Methods: We performed a retrospective cohort study of patients who underwent colonoscopy with polypectomy at a safety-net healthcare system before (n=1,822) and after (n=1,320) implementation of CoRS in December 2013. Recommendations were classified as guideline-adherent or nonadherent according to the US Multi-Society Task Force on CRC. We defined surveillance recommendations shorter and longer than guideline recommendations as potential overuse and underuse, respectively. We used multivariable generalized linear mixed models to identify correlates of guideline-adherent recommendations. Results: The proportion of guideline-adherent surveillance recommendations was significantly higher post-CoRS than pre-CoRS (84.6% vs 77.4%; P<.001), with fewer recommendations for potential overuse and underuse. In the post-CoRS period, CoRS was used for 89.8% of cases and, compared with cases for which it was not used, was associated with a higher proportion of guideline-adherent recommendations (87.0% vs 63.4%; RR, 1.34; 95% CI, 1.23-1.42). In multivariable analysis, surveillance recommendations were also more likely to be guideline-adherent in patients with adenomas but less likely among those with fair bowel preparation and those with family history of CRC. Of 203 nonadherent recommendations, 70.4% were considered potential overuse, 20.2% potential underuse, and 9.4% were not provided surveillance recommendations. Conclusions: An EMR-based CoRS was widely used and significantly improved guideline adherence of surveillance recommendations.
Copyright © 2018 by the National Comprehensive Cancer Network.
Conflict of interest statement
Dr. Gupta has disclosed that he is a consultant for Boston Scientific. The remaining authors have disclosed that they have no financial interests, arrangements, affiliations, or commercial interests with the manufacturers of any products discussed in this article or their competitors.
Figures
Similar articles
-
Predictors of guideline concordance for surveillance colonoscopy recommendations in patients at a safety-net health system.Cancer Causes Control. 2015 Nov;26(11):1653-60. doi: 10.1007/s10552-015-0661-x. Epub 2015 Sep 16. Cancer Causes Control. 2015. PMID: 26376891 Free PMC article.
-
Post-polypectomy Guideline Adherence: Importance of Belief in Guidelines, Not Guideline Knowledge or Fear of Missed Cancer.Dig Dis Sci. 2015 Oct;60(10):2937-45. doi: 10.1007/s10620-015-3685-x. Epub 2015 May 7. Dig Dis Sci. 2015. PMID: 25947332 Free PMC article. Review.
-
Physician Non-adherence to Colonoscopy Interval Guidelines in the Veterans Affairs Healthcare System.Gastroenterology. 2015 Oct;149(4):938-51. doi: 10.1053/j.gastro.2015.06.026. Epub 2015 Jun 26. Gastroenterology. 2015. PMID: 26122143
-
[Impact of implementation strategies on adherence rates to colorectal cancer (CRC) guidelines after polypectomy in a university hospital].Z Gastroenterol. 2013 Oct;51(10):1157-64. doi: 10.1055/s-0033-1335081. Epub 2013 Oct 11. Z Gastroenterol. 2013. PMID: 24122376 Clinical Trial. German.
-
Adherence to post-polypectomy surveillance guidelines: a systematic review and meta-analysis.Endoscopy. 2019 Jul;51(7):673-683. doi: 10.1055/a-0865-2082. Epub 2019 Mar 25. Endoscopy. 2019. PMID: 30909308
Cited by
-
The Effect of an EHR Order Set on Cancer Screening Order Rates in Community-Based Health Centers.Appl Clin Inform. 2025 May;16(3):496-506. doi: 10.1055/a-2524-5076. Epub 2025 Jun 4. Appl Clin Inform. 2025. PMID: 40467470 Free PMC article.
-
Clinician based decision tool to guide recommended interval between colonoscopies: development and evaluation pilot study.BMC Med Inform Decis Mak. 2022 May 17;22(1):136. doi: 10.1186/s12911-022-01872-z. BMC Med Inform Decis Mak. 2022. PMID: 35581662 Free PMC article.
-
Implementing a closed loop clinical decision support system for sustainable preoperative care.NPJ Digit Med. 2025 Jan 3;8(1):6. doi: 10.1038/s41746-024-01371-7. NPJ Digit Med. 2025. PMID: 39753745 Free PMC article.
-
Measuring and Improving Quality of Colonoscopy for Colorectal Cancer Screening.Tech Innov Gastrointest Endosc. 2022;24(3):269-283. doi: 10.1016/j.tige.2021.11.002. Epub 2021 Nov 14. Tech Innov Gastrointest Endosc. 2022. PMID: 36778081 Free PMC article.
-
Traditional and Novel Colonoscopy Quality Metrics: What's Important in 2025.Curr Gastroenterol Rep. 2025 Aug 8;27(1):58. doi: 10.1007/s11894-025-01006-1. Curr Gastroenterol Rep. 2025. PMID: 40775559 Review.
References
-
- US Preventive Services Task Force. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. Ann Intern Med 2008;149:627–637. - PubMed
-
- Lieberman DA, de Garmo PL, Fleischer DE, et al. Patterns of endoscopy use in the United States. Gastroenterology 2000;118:619–624. - PubMed
-
- Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2012;143:844–857. - PubMed
-
- Saini SD, Schoenfeld P, Vijan S. Surveillance colonoscopy is cost-effective for patients with adenomas who are at high risk of colorectal cancer. Gastroenterology 2010;138:2292–2299.e2291. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
