

Prospective, Multisite, International Comparison of 18F-Fluoromethylcholine PET/CT, Multiparametric MRI, and 68Ga-HBED-CC PSMA-11 PET/CT in Men with High-Risk Features and Biochemical Failure After Radical Prostatectomy: Clinical Performance and Patient Outcomes
- PMID: 30442757
- PMCID: PMC6581227
- DOI: 10.2967/jnumed.118.220103
Prospective, Multisite, International Comparison of 18F-Fluoromethylcholine PET/CT, Multiparametric MRI, and 68Ga-HBED-CC PSMA-11 PET/CT in Men with High-Risk Features and Biochemical Failure After Radical Prostatectomy: Clinical Performance and Patient Outcomes
Abstract
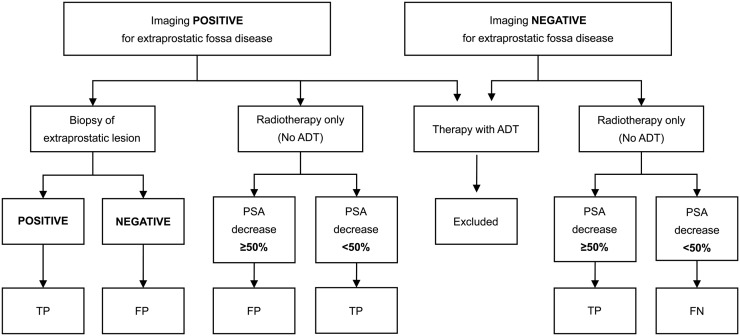
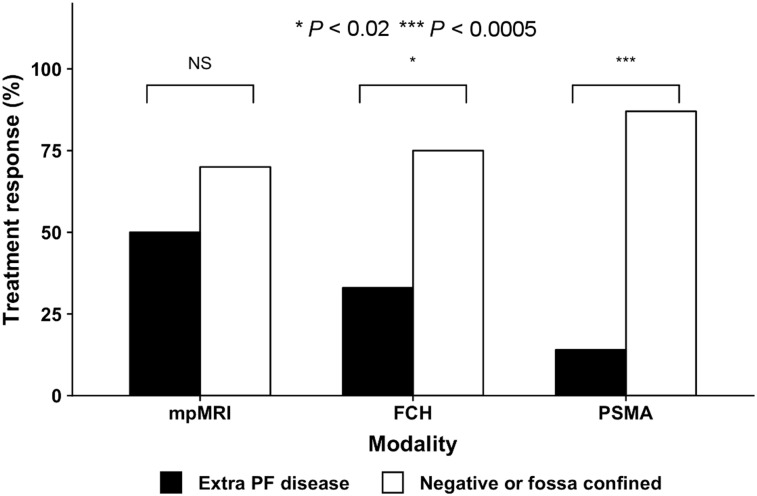
A significant proportion of men with rising prostate-specific antigen (PSA) levels after radical prostatectomy (RP) fail prostate fossa (PF) salvage radiation treatment (SRT). This study was done to assess the ability of 18F-fluoromethylcholine (18F-FCH) PET/CT (hereafter referred to as 18F-FCH), 68Ga-HBED-CC PSMA-11 PET/CT (hereafter referred to as PSMA), and pelvic multiparametric MRI (hereafter referred to as pelvic MRI) to identify men who will best benefit from SRT. Methods: Prospective, multisite imaging studies were carried out in men who had rising PSA levels after RP, high-risk features, and negative/equivocal conventional imaging results and who were being considered for SRT. 18F-FCH (91/91), pelvic MRI (88/91), and PSMA (31/91) (Australia) were all performed within 2 wk. Imaging was interpreted by experienced local/central interpreters who were masked with regard to other imaging results, with consensus being reached for discordant interpretations. Expected management was documented before and after imaging, and data about all treatments and PSA levels were collected for 3 y. The treatment response to SRT was defined as a reduction in PSA levels of >50% without androgen deprivation therapy. Results: The median Gleason score, PSA level at imaging, and PSA doubling time were 8, 0.42 (interquartile range, 0.29-0.93) ng/mL, and 5.0 (interquartile range, 3.3-7.6) months. Recurrent prostate cancer was detected in 28% (25/88) by pelvic MRI, 32% (29/91) by 18F-FCH, and 42% (13/31) by PSMA. This recurrence was found within the PF in 21.5% (19/88), 13% (12/91), and 19% (6/31) and at sites outside the PF (extra-PF) in 8% (7/88), 19% (17/91), and 32% (10/31) by MRI, 18F-FCH, and PSMA, respectively (P < 0.004). A total of 94% (16/17) of extra-PF sites on 18F-FCH were within the pelvic MRI field. Intrapelvic extra-PF disease was detected in 90% (9/10) by PSMA and in 31% (5/16) by MRI. 18F-FCH changed management in 46% (42/91), and MRI changed management in 24% (21/88). PSMA provided additional management changes over 18F-FCH in 23% (7/31). The treatment response to SRT was higher in men with negative results or disease confined to the PF than in men with extra-PF disease (18F-FCH 73% [32/44] versus 33% [3/9] [P < 0.02], pelvic MRI 70% [32/46] versus 50% [2/4] [P was not significant], and PSMA 88% [7/8] versus 14% [1/7] [P < 0.005]). Men with negative imaging results (MRI, 18F-FCH, or PSMA) had high (78%) SRT response rates. Conclusion:18F-FCH and PSMA had high detection rates for extra-PF disease in men with negative/equivocal conventional imaging results and rising PSA levels after RP. These findings affected management and treatment responses, suggesting an important role for PET in triaging men being considered for curative SRT.
Keywords: 18F-fluoromethylcholine; PET; PSMA; biochemical recurrence; multiparametric MRI; prostate cancer.
© 2019 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Stephenson AJ, Slawin KM, Bianco FJ, Jr, Scardino PT. Perspectives on the natural history of recurrent prostate cancer after radical prostatectomy, based on the response to salvage radiotherapy. BJU Int. 2004;94:1210–1212. - PubMed
-
- Carrie C, Hasbini A, de Laroche G, et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): a randomised, multicentre, open-label phase 3 trial. Lancet Oncol. 2016;17:747–756. - PubMed
-
- Tendulkar RD, Agrawal S, Gao T, et al. Contemporary update of a multi-institutional predictive nomogram for salvage radiotherapy after radical prostatectomy. J Clin Oncol. 2016;34:3648–3654. - PubMed
-
- van Leeuwen PJ, Emmett L, Ho B, et al. Prospective evaluation of 68Gallium-prostate-specific membrane antigen positron emission tomography/computed tomography for preoperative lymph node staging in prostate cancer. BJU Int. 2017;119:209–215. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous