

Uptake and Clinical Utility of Multibiomarker Disease Activity Testing in the United States
- PMID: 30442830
- PMCID: PMC6411282
- DOI: 10.3899/jrheum.180071
Uptake and Clinical Utility of Multibiomarker Disease Activity Testing in the United States
Abstract
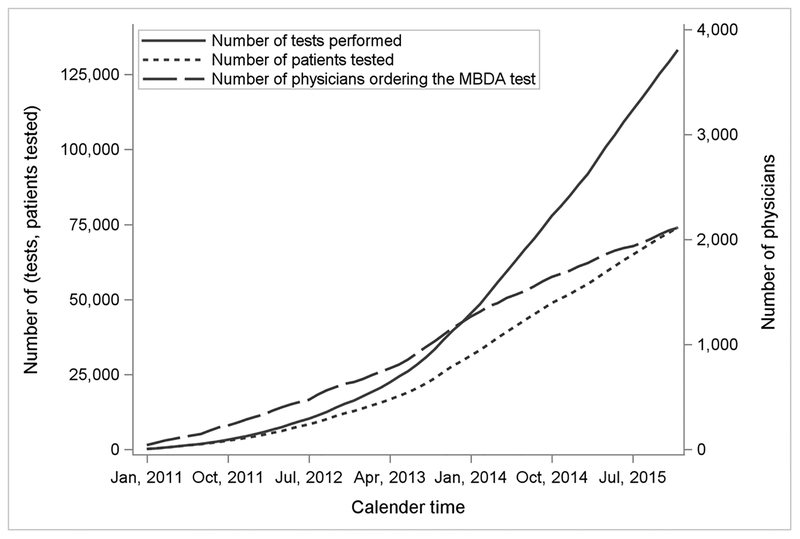
Objective: The clinical utility of the multibiomarker disease activity (MBDA) test for rheumatoid arthritis (RA) management in routine care in the United States has not been thoroughly studied.
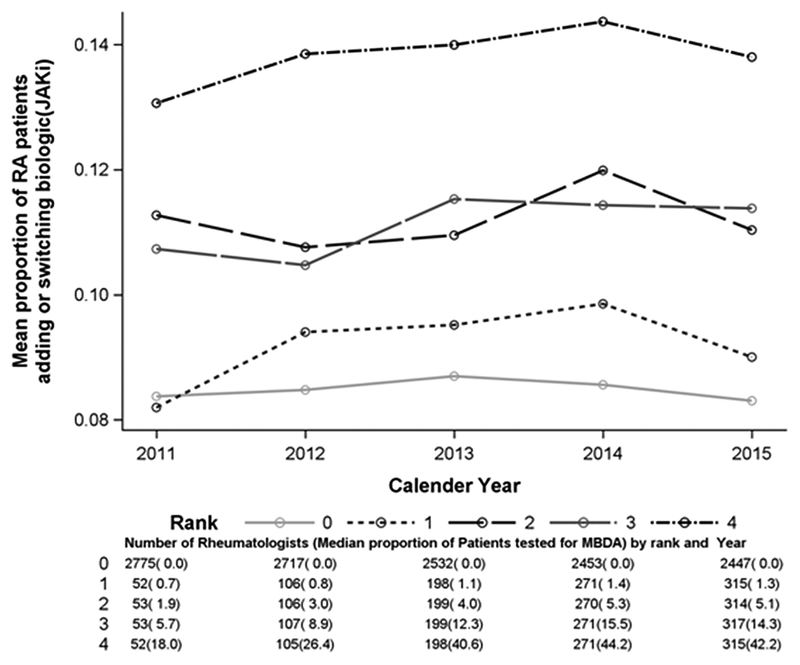
Methods: Using 2011-2015 Medicare data, we linked each patient with RA to their MBDA test result. Initiation of a biologic or Janus kinase (JAK) inhibitor in the 6 months following MBDA testing was described. Multivariable adjustment evaluated the likelihood of adding or switching biologic/JAK inhibitor, controlling for potential confounders. For patients with high MBDA scores who added a new RA therapy and were subsequently retested, lack of improvement in the MBDA score was evaluated as a predictor of future RA medication failure, defined by the necessity to change RA medications again.
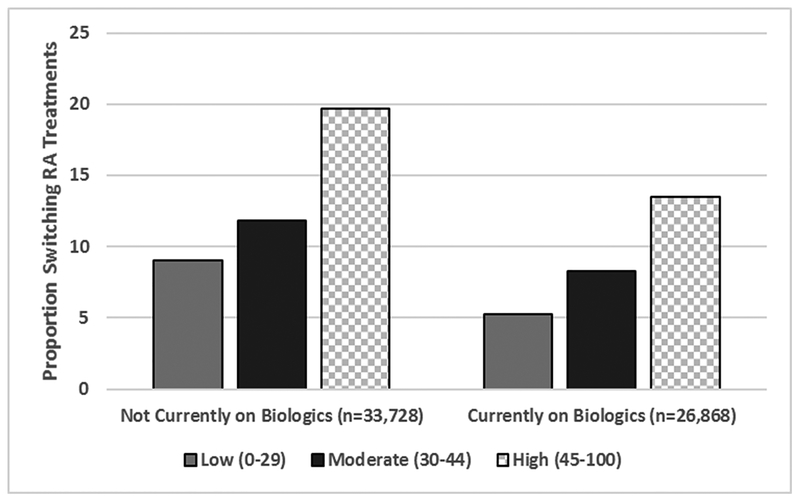
Results: Among 60,596 RA patients with MBDA testing, the proportion adding or switching biologics/JAK inhibitor among those not already taking a biologic/JAK inhibitor was 9.0% (low MBDA), 11.8% (moderate MBDA), and 19.7% (high MBDA, p < 0.0001). Similarly, among those already taking biologics/JAK inhibitor, the proportions were 5.2%, 8.3%, and 13.5% (p < 0.0001). After multivariable adjustment, referent to those with low disease MBDA scores, the likelihood of switching was 1.51-fold greater (95% CI 1.35-1.69) for patients with moderate MBDA scores, and 2.62 (2.26-3.05) for patients with high MBDA scores. Among those with high MBDA scores who subsequently added a biologic/JAK inhibitor and were retested, lack of improvement in the MBDA score category was associated with likelihood of future RA treatment failure (OR 1.61, 95% CI 1.27-2.03).
Conclusion: The MBDA score was associated with both biologic and JAK inhibitor medication addition/switching and subsequent treatment outcomes.
Keywords: BIOLOGICS; BIOMARKER; MEDICATION PERSISTENCE; MEDICATION SWITCHING; RHEUMATOID ARTHRITIS.
Figures
Similar articles
-
Multibiomarker disease activity score and C-reactive protein in a cross-sectional observational study of patients with rheumatoid arthritis with and without concomitant fibromyalgia.Rheumatology (Oxford). 2016 Apr;55(4):640-8. doi: 10.1093/rheumatology/kev388. Epub 2015 Nov 25. Rheumatology (Oxford). 2016. PMID: 26608972 Free PMC article.
-
Cost-effective Tapering Algorithm in Patients with Rheumatoid Arthritis: Combination of Multibiomarker Disease Activity Score and Autoantibody Status.J Rheumatol. 2019 May;46(5):460-466. doi: 10.3899/jrheum.180028. Epub 2018 Dec 1. J Rheumatol. 2019. PMID: 30504510 Clinical Trial.
-
Prediction of disease relapses by multibiomarker disease activity and autoantibody status in patients with rheumatoid arthritis on tapering DMARD treatment.Ann Rheum Dis. 2016 Sep;75(9):1637-44. doi: 10.1136/annrheumdis-2015-207900. Epub 2015 Oct 19. Ann Rheum Dis. 2016. PMID: 26483255 Free PMC article. Clinical Trial.
-
Multibiomarker disease activity score: an objective tool for monitoring rheumatoid arthritis? A systematic review and meta-analysis.Rheumatology (Oxford). 2023 Jun 1;62(6):2048-2059. doi: 10.1093/rheumatology/keac715. Rheumatology (Oxford). 2023. PMID: 36575983 Free PMC article.
-
Cardiovascular Safety of Biologics and JAK Inhibitors in Patients with Rheumatoid Arthritis.Curr Rheumatol Rep. 2018 May 30;20(7):42. doi: 10.1007/s11926-018-0752-2. Curr Rheumatol Rep. 2018. PMID: 29846814 Review.
Cited by
-
Derivation and internal validation of a multi-biomarker-based cardiovascular disease risk prediction score for rheumatoid arthritis patients.Arthritis Res Ther. 2020 Dec 4;22(1):282. doi: 10.1186/s13075-020-02355-0. Arthritis Res Ther. 2020. PMID: 33276814 Free PMC article.
-
Biomarker discovery studies for patient stratification using machine learning analysis of omics data: a scoping review.BMJ Open. 2021 Dec 6;11(12):e053674. doi: 10.1136/bmjopen-2021-053674. BMJ Open. 2021. PMID: 34873011 Free PMC article.
References
-
- Singh JA, Saag KG, Bridges SL Jr., Akl EA, Bannuru RR, Sullivan MC, Vaysbrot E, McNaughton C, Osani M, Shmerling RH et al.: 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & rheumatology 2016, 68(1):1–26. - PubMed
-
- Scott IC, Scott DL: Joint counts in inflammatory arthritis. Clin Exp Rheumatol 2014, 32(5 Suppl 85):S-7–12. - PubMed
-
- Curtis JR, Churchill M, Kivitz A, Samad A, Gauer L, Gervitz L, Koetse W, Melin J, Yazici Y: A Randomized Trial Comparing Disease Activity Measures for the Assessment and Prediction of Response in Rheumatoid Arthritis Patients Initiating Certolizumab Pegol. Arthritis & rheumatology 2015, 67(12):3104–3112. - PMC - PubMed
-
- Lee YC, Hackett J, Frits M, Iannaccone CK, Shadick NA, Weinblatt ME, Segurado OG, Sasso EH: Multibiomarker disease activity score and C-reactive protein in a cross-sectional observational study of patients with rheumatoid arthritis with and without concomitant fibromyalgia. Rheumatology (Oxford) 2015. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical