

A nutrition problem solved by a two-step endoscopic removal of a non-adjustable gastric band
- PMID: 30443320
- PMCID: PMC6232287
- DOI: 10.1093/jscr/rjy306
A nutrition problem solved by a two-step endoscopic removal of a non-adjustable gastric band
Abstract
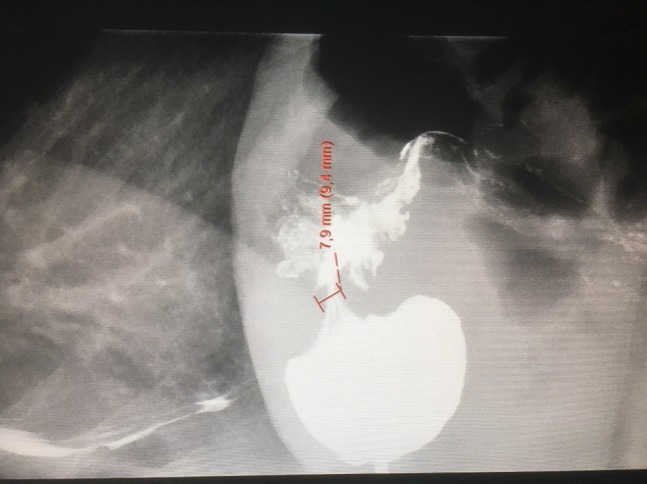
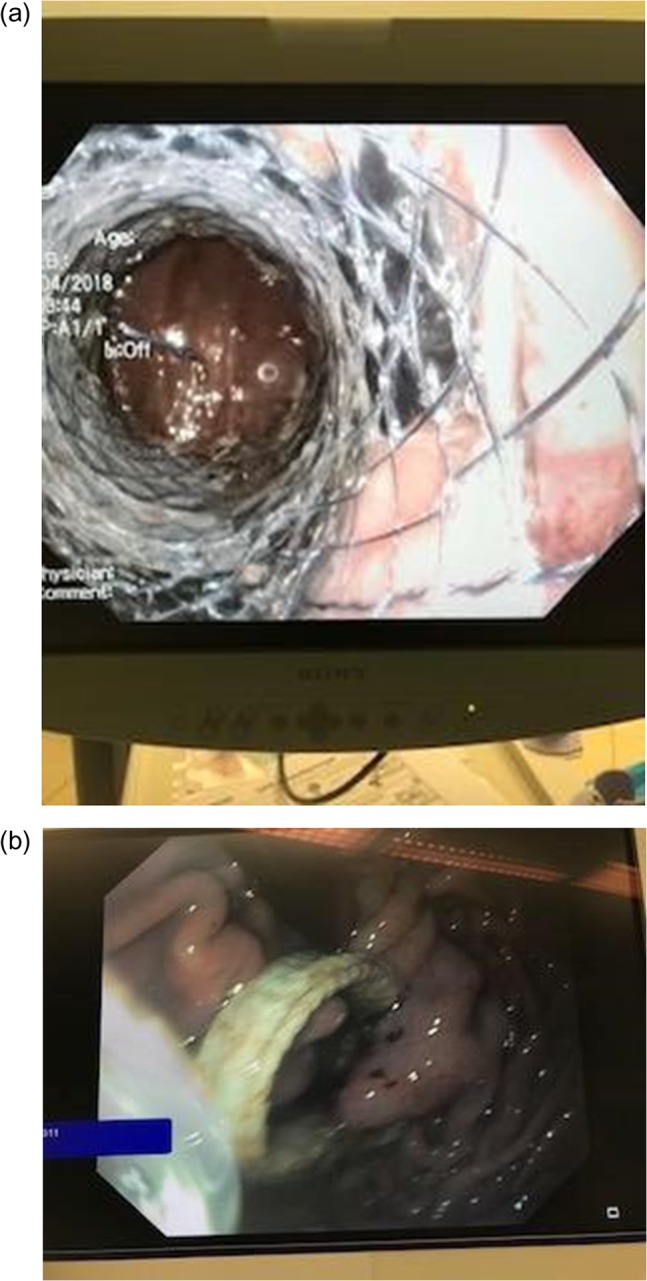
Bariatric surgery is an effective approach for weight loss and short-term improvement in metabolic disorders. Stenosis is a common complication of gastric banding. Balloon dilatation or gastrotomy has been employed in this setting. Few studies have indicated endoscopic removal of the band a feasible procedure. We present a 60-year-old female who underwent gastric banding in 1985 and suffered from late stenosis and malnutrition. Endoscopy revealed a severe stenosis. A two-step procedure was performed. Initially a coated stent was placed into the stenosis to achieve pressure necrosis. Two weeks later, the stent was removed and the band was removed endoscopically. The procedure was performed without any complications. The patient was discharged the next day. A follow-up after 2 months revealed no problems with stenosis or malnutrition. The procedure was a safe, efficient and convenient way of handling late stenosis after gastric banding.
Figures
Similar articles
-
Long-term results of adjustable gastric banding in a cohort of 186 super-obese patients with a BMI≥ 50 kg/m2.J Visc Surg. 2012 Apr;149(2):e143-52. doi: 10.1016/j.jviscsurg.2012.01.007. Epub 2012 Mar 2. J Visc Surg. 2012. PMID: 22386891 Clinical Trial.
-
Endoscopic management of post-laparoscopic sleeve gastrectomy stenosis.Surg Endosc. 2018 Feb;32(2):601-609. doi: 10.1007/s00464-017-5709-4. Epub 2017 Jul 19. Surg Endosc. 2018. PMID: 28726143
-
Revisional bariatric surgery after failed laparoscopic adjustable gastric banding - a single-center, long-term retrospective study.Wideochir Inne Tech Maloinwazyjne. 2017;12(1):32-36. doi: 10.5114/wiitm.2017.66671. Epub 2017 Mar 22. Wideochir Inne Tech Maloinwazyjne. 2017. PMID: 28446930 Free PMC article.
-
Laparoscopic sleeve gastrectomy as revisional surgery for adjustable gastric band erosion.J Laparoendosc Adv Surg Tech A. 2014 Sep;24(9):593-600. doi: 10.1089/lap.2013.0584. Epub 2014 Jul 29. J Laparoendosc Adv Surg Tech A. 2014. PMID: 25072398
-
[Surgery for morbid obesity: 2. Complications. Results of a Technologic Evaluation by the ANAES].J Chir (Paris). 2003 Feb;140(1):4-21. J Chir (Paris). 2003. PMID: 12709648 Review. French.
References
-
- Reges O, Greenland P, Dicker D, Leibowitz M, Hoshen M, Gofer I, et al. . Association of bariatric surgery using laparoscopic banding, Roux-en-Y gastric bypass, or laparoscopic sleeve gastrectomy vs. usual care obesity management with all-cause mortality. J Am Med Assoc 2018;319:279–90. 10.1001/jama.2017.20513. - DOI - PMC - PubMed
-
- Puig CA, Waked TM, Baron TH Sr, Wong Kee Song LM, Gutierrez J, Sarr MG. The role of endoscopic stents in the management of chronic anastomotic and staple line leaks and chronic strictures after bariatric surgery. Surg Obes Relat Dis 2014;10:613–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
