

Risk Factors for Postoperative Coronal Balance in Adult Spinal Deformity Surgery
- PMID: 30443478
- PMCID: PMC6232708
- DOI: 10.1177/2192568218764904
Risk Factors for Postoperative Coronal Balance in Adult Spinal Deformity Surgery
Abstract
Study design: A retrospective case-control study.
Objectives: To determine factors influencing the ability to achieve coronal balance following spinal deformity surgery.
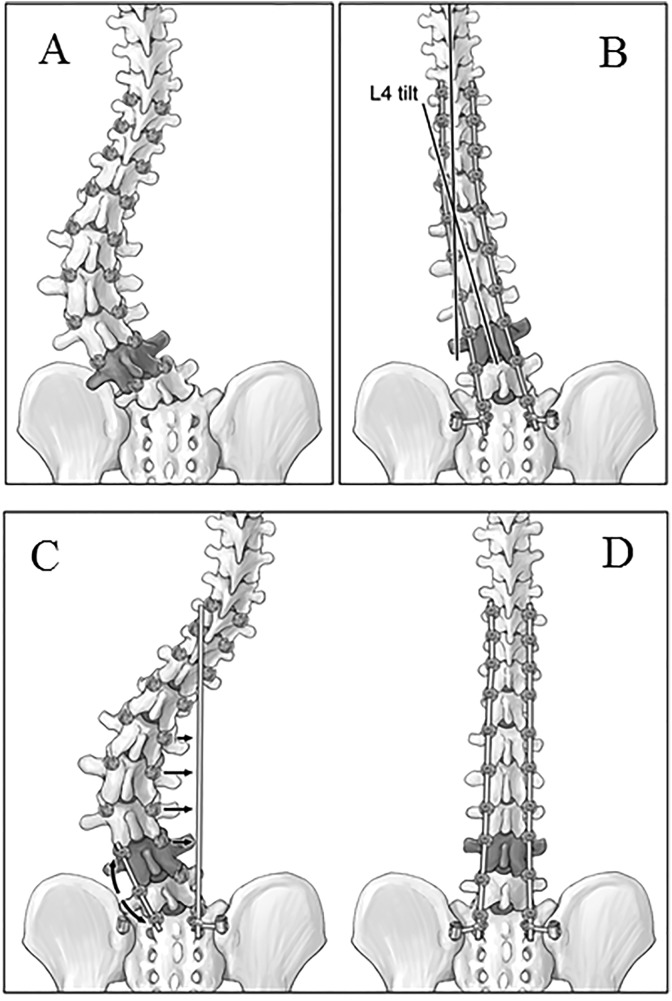
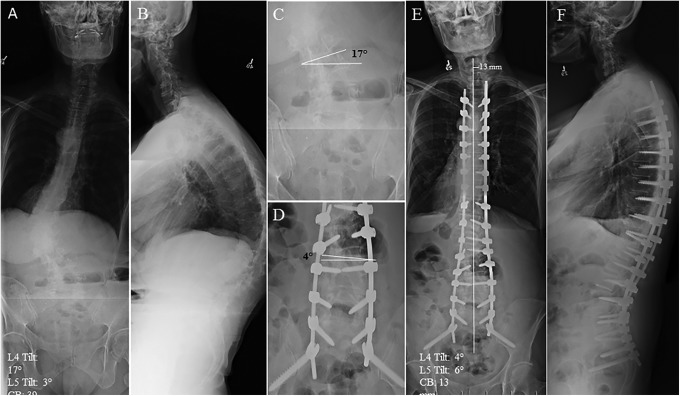
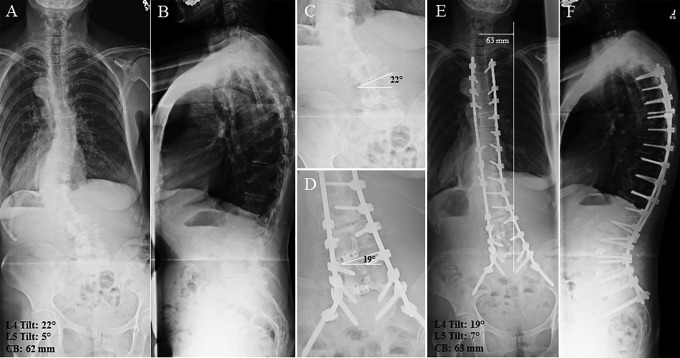
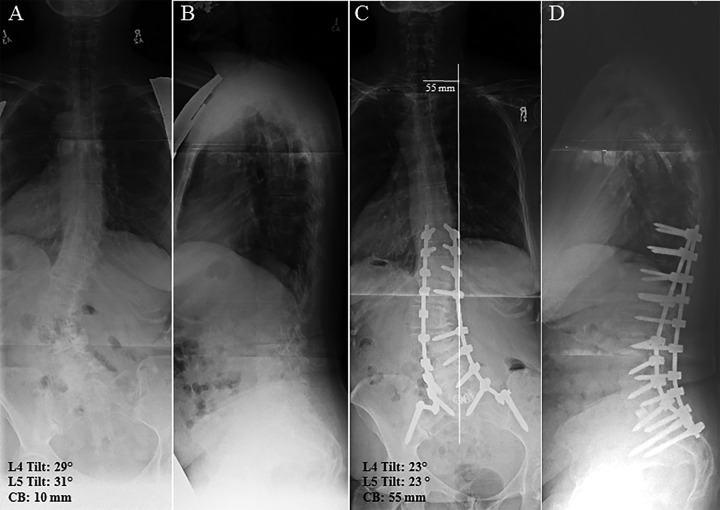
Methods: Following institutional ethics approval, the radiographs of 47 patients treated for spinal deformity surgery with long fusions to the pelvis, were retrospectively reviewed. The postoperative measurements included coronal balance, L4 tilt, and L5 tilt, levels fused, apical vertebral translation and maximum Cobb angle. L4 and L5 tilt angles were measured between the superior endplate and the horizontal. Sagittal parameters including thoracic kyphosis, lumbar lordosis, pelvic incidence, and sagittal vertical axis were recorded. Coronal balance was defined as the distance between the central sacral line and the mid body of C7 being ≤40 mm. Surgical factors, including levels fused, use of iliac fixation with and without connectors, use of S2A1 screws, interbody devices, and osteotomies. Statistical tests were performed to determine factors that contribute to postoperative coronal imbalance.
Results: Of the 47 patients reviewed, 32 were balanced after surgery and 14 were imbalanced. Coronal balance was 1.30 cm from center in the balanced group compared to 4.83 cm in the imbalanced group (P < .01). Both L4 and L5 tilt were statistically different between the groups. Gender and the use of transverse connectors differed between the groups but not statistically.
Conclusions: In adult spinal deformity patients undergoing primary fusions to the pelvis, the ability to level the coronal tilt of L4 and L5 had the greatest impact on the ability to achieve coronal balance in this small series. A larger prospective series can help validate this important finding.
Keywords: L4 tilt; L5 tilt; adult spinal deformity; coronal balance; pelvic fixation; sagittal balance.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SJL serves as a consultant to Stryker, Medtronic, and AOSpine and receives money for travel, conferences, and teaching from Stryker, Medtronic, AOSpine, Depuy, and L&K.
Figures

Similar articles
-
Coronal T1 Pelvic Tilt, a Novel Predictive Index for Global Coronal Alignment in Adult Spinal Deformity.Spine (Phila Pa 1976). 2020 Oct 1;45(19):1335-1340. doi: 10.1097/BRS.0000000000003522. Spine (Phila Pa 1976). 2020. PMID: 32355135
-
Utility of multilevel lateral interbody fusion of the thoracolumbar coronal curve apex in adult deformity surgery in combination with open posterior instrumentation and L5-S1 interbody fusion: a case-matched evaluation of 32 patients.J Neurosurg Spine. 2017 Feb;26(2):208-219. doi: 10.3171/2016.8.SPINE151543. Epub 2016 Oct 21. J Neurosurg Spine. 2017. PMID: 27767682
-
Coronal Spinal Balance in Adult Spine Deformity Patients With Long Spinal Fusions: A Minimum 2- to 5-Year Follow-up Study.J Spinal Disord Tech. 2015 Nov;28(9):341-7. doi: 10.1097/BSD.0b013e3182aab2ff. J Spinal Disord Tech. 2015. PMID: 24077418
-
The importance of spino-pelvic balance in L5-s1 developmental spondylolisthesis: a review of pertinent radiologic measurements.Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S27-34. doi: 10.1097/01.brs.0000155560.92580.90. Spine (Phila Pa 1976). 2005. PMID: 15767882 Review.
-
Biomechanical analysis of the spino-pelvic organization and adaptation in pathology.Eur Spine J. 2011 Sep;20 Suppl 5(Suppl 5):609-18. doi: 10.1007/s00586-011-1928-x. Epub 2011 Aug 2. Eur Spine J. 2011. PMID: 21809016 Free PMC article. Review.
Cited by
-
Risk Factors for Immediate Postoperative Coronal Imbalance in Degenerative Lumbar Scoliosis Patients Fused to Pelvis.Global Spine J. 2021 Jun;11(5):649-655. doi: 10.1177/2192568220917648. Epub 2020 Apr 8. Global Spine J. 2021. PMID: 32875894 Free PMC article.
-
The odontoid-CSVL distance in a global population of asymptomatic volunteers: normative values and implications for spinal coronal alignment.Eur Spine J. 2021 Dec;30(12):3639-3646. doi: 10.1007/s00586-021-06873-6. Epub 2021 May 19. Eur Spine J. 2021. PMID: 34009398
-
Be Prepared: Preoperative Coronal Malalignment Often Leads to More Extensive Surgery Than Sagittal Malalignment During Adult Spinal Deformity Surgery.Neurospine. 2021 Sep;18(3):570-579. doi: 10.14245/ns.2142384.192. Epub 2021 Sep 30. Neurospine. 2021. PMID: 34610688 Free PMC article.
-
Posterior column osteotomy plus unilateral cage strutting for correction of lumbosacral fractional curve in degenerative lumbar scoliosis.J Orthop Surg Res. 2020 Oct 20;15(1):482. doi: 10.1186/s13018-020-02011-y. J Orthop Surg Res. 2020. PMID: 33081812 Free PMC article.
-
Postoperative Radiological Improvement after Staged Surgery Using Lateral Lumbar Interbody Fusion for Preoperative Coronal Malalignment in Patients with Adult Spinal Deformity.J Clin Med. 2023 Mar 20;12(6):2389. doi: 10.3390/jcm12062389. J Clin Med. 2023. PMID: 36983389 Free PMC article.
References
-
- Aebi M. The adult scoliosis. Eur Spine J. 2005;14:925–948. - PubMed
-
- Bradford DS, Tay BKB, Hu SS. Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine (Phila Pa 1976). 1999;24:2617–2629. - PubMed
-
- Oskouian RJ, Jr, Shaffrey CI. Degenerative lumbar scoliosis. Neurosurg Clin N Am. 2006;17:299–315. - PubMed
-
- Acaroglu E, Guler UO, Olgun ZD, et al. ; European Spine Study Group. Multiple regression analysis of factors affecting health-related quality of life in adult spinal deformity. Spine Deform. 2015;3:360–366. - PubMed
-
- Birknes JK, White AP, Albert TJ, Shaffrey CI, Harrop JS. Adult degenerative scoliosis: a review. Neurosurgery. 2008;63(3 suppl):94–103. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
