

Targeting low-normal or high-normal mean arterial pressure after cardiac arrest and resuscitation: a randomised pilot trial
- PMID: 30443729
- PMCID: PMC6280836
- DOI: 10.1007/s00134-018-5446-8
Targeting low-normal or high-normal mean arterial pressure after cardiac arrest and resuscitation: a randomised pilot trial
Abstract
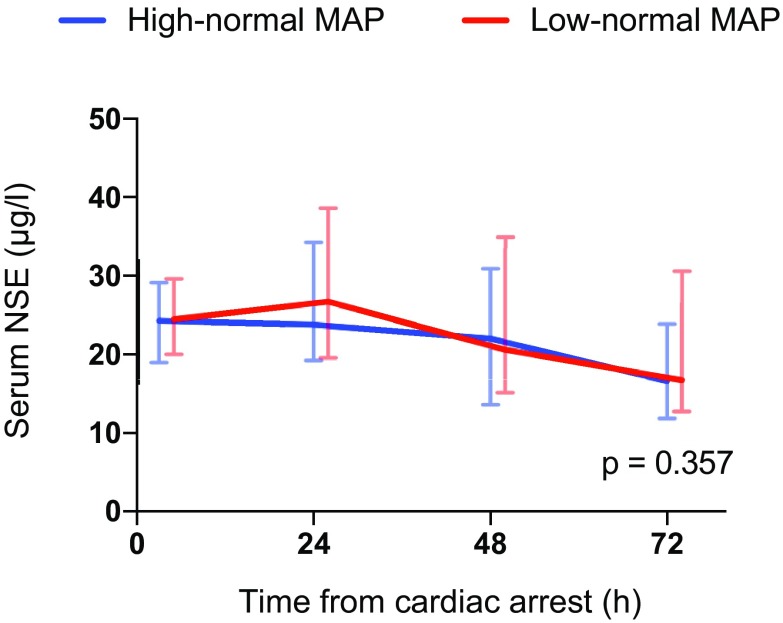
Purpose: We aimed to determine the feasibility of targeting low-normal or high-normal mean arterial pressure (MAP) after out-of-hospital cardiac arrest (OHCA) and its effect on markers of neurological injury.
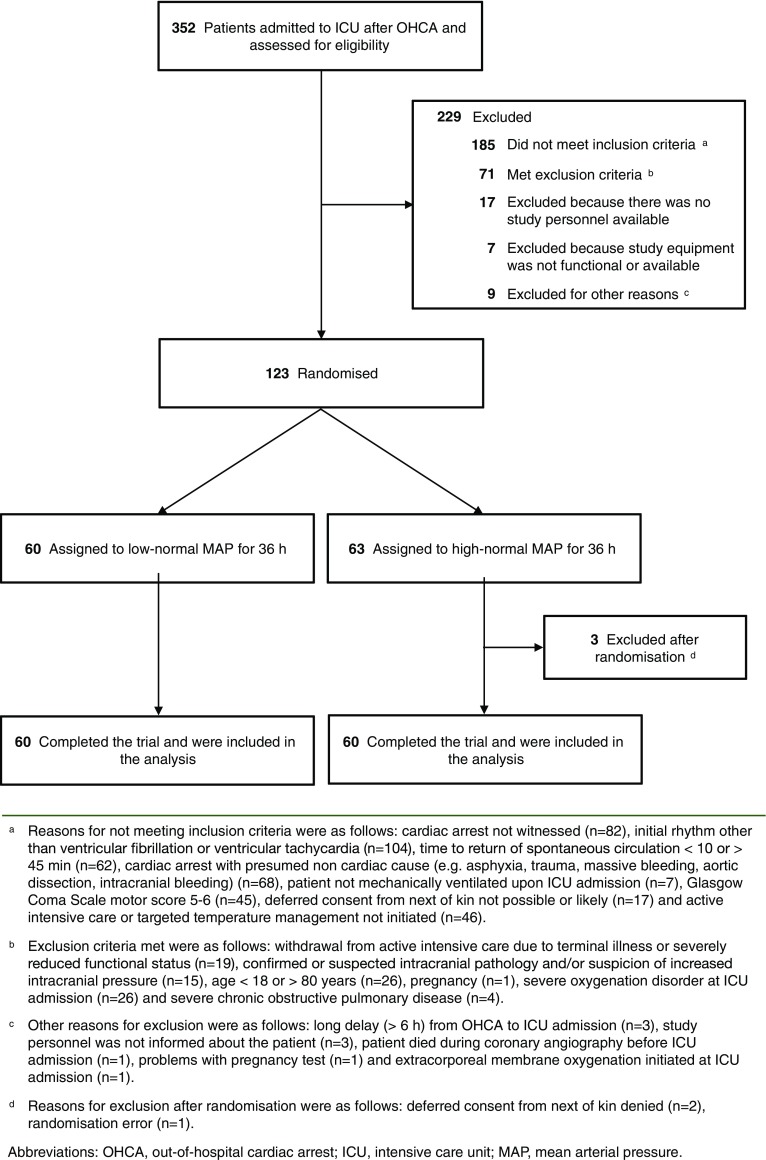
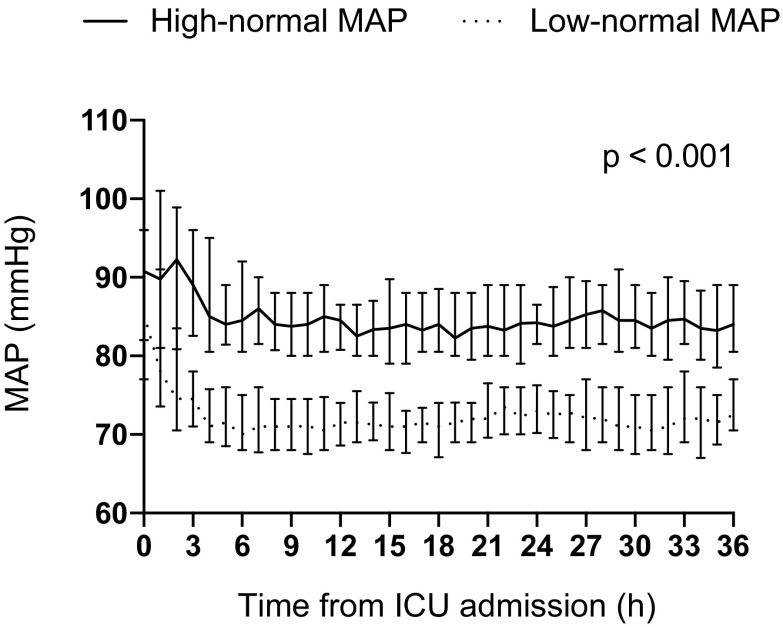
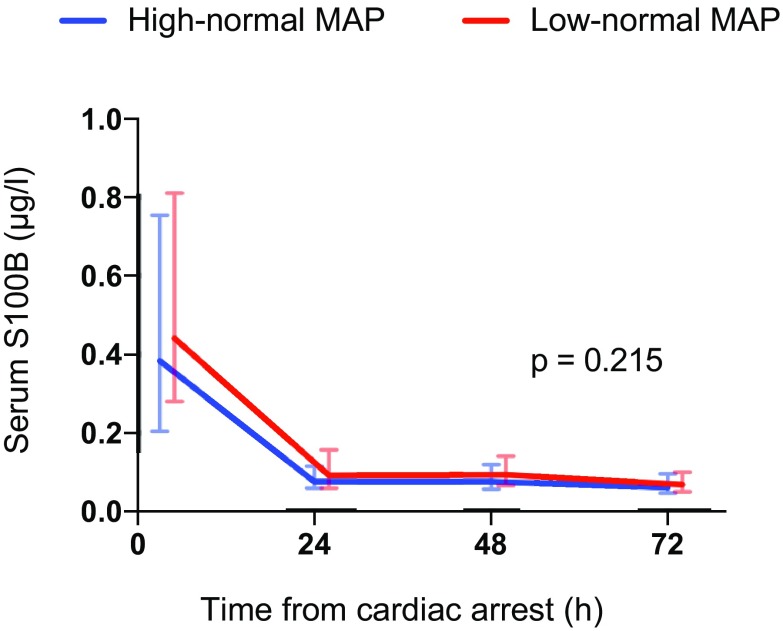
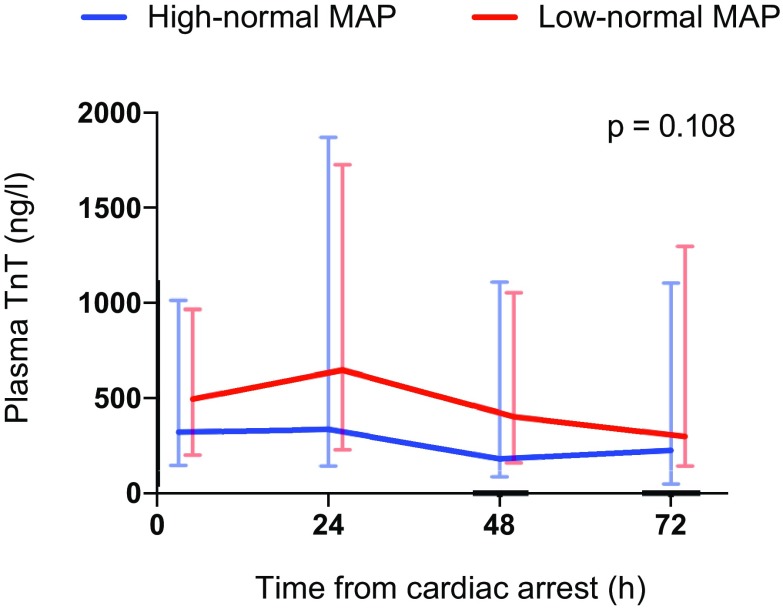
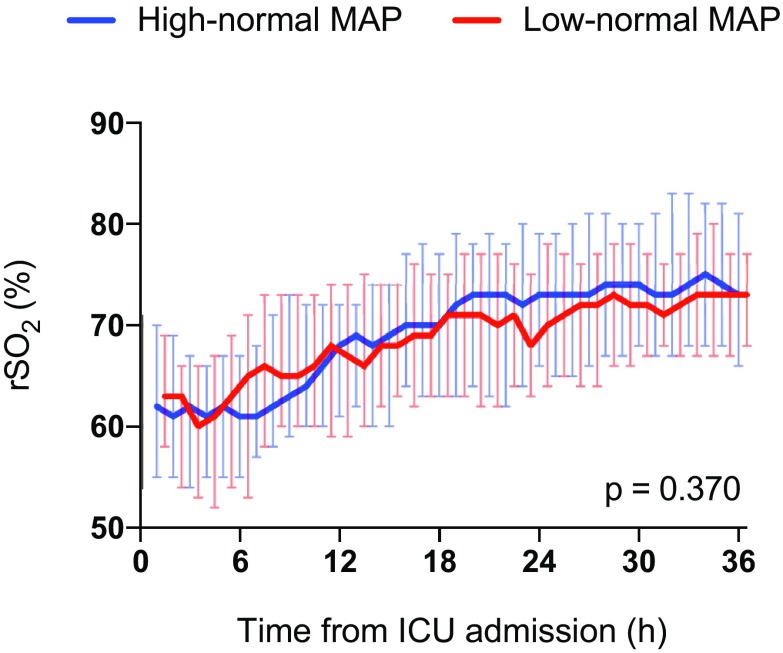
Methods: In the Carbon dioxide, Oxygen and Mean arterial pressure After Cardiac Arrest and REsuscitation (COMACARE) trial, we used a 23 factorial design to randomly assign patients after OHCA and resuscitation to low-normal or high-normal levels of arterial carbon dioxide tension, to normoxia or moderate hyperoxia, and to low-normal or high-normal MAP. In this paper we report the results of the low-normal (65-75 mmHg) vs. high-normal (80-100 mmHg) MAP comparison. The primary outcome was the serum concentration of neuron-specific enolase (NSE) at 48 h after cardiac arrest. The feasibility outcome was the difference in MAP between the groups. Secondary outcomes included S100B protein and cardiac troponin (TnT) concentrations, electroencephalography (EEG) findings, cerebral oxygenation and neurological outcome at 6 months after cardiac arrest.
Results: We recruited 123 patients and included 120 in the final analysis. We found a clear separation in MAP between the groups (p < 0.001). The median (interquartile range) NSE concentration at 48 h was 20.6 µg/L (15.2-34.9 µg/L) in the low-normal MAP group and 22.0 µg/L (13.6-30.9 µg/L) in the high-normal MAP group, p = 0.522. We found no differences in the secondary outcomes.
Conclusions: Targeting a specific range of MAP was feasible during post-resuscitation intensive care. However, the blood pressure level did not affect the NSE concentration at 48 h after cardiac arrest, nor any secondary outcomes.
Keywords: Arterial pressure; Cardiac arrest; Hypoxic ischemic encephalopathy; Intensive care; Mechanical ventilation; Neuron-specific enolase (NSE).
Figures
Comment in
-
NSE concentrations and haemolysis after cardiac arrest.Intensive Care Med. 2019 May;45(5):741-742. doi: 10.1007/s00134-019-05547-8. Epub 2019 Feb 13. Intensive Care Med. 2019. PMID: 30758520 No abstract available.
References
-
- Adrie C, Adib-Conquy M, Laurent I, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106:562–568. doi: 10.1161/01.CIR.0000023891.80661.AD. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
