

Predictors of all-cause mortality and ischemic events within and beyond 1 year after an acute coronary syndrome: Results from the EPICOR registry
- PMID: 30443916
- PMCID: PMC6436503
- DOI: 10.1002/clc.23116
Predictors of all-cause mortality and ischemic events within and beyond 1 year after an acute coronary syndrome: Results from the EPICOR registry
Abstract
Background: Patients discharged after an acute coronary syndrome (ACS) have substantial risk of recurrent ischemic events or dying.
Hypothesis: A difference may exist in risk predictors for all-cause mortality and ischemic events between year 1 and 2 of follow-up post-ACS.
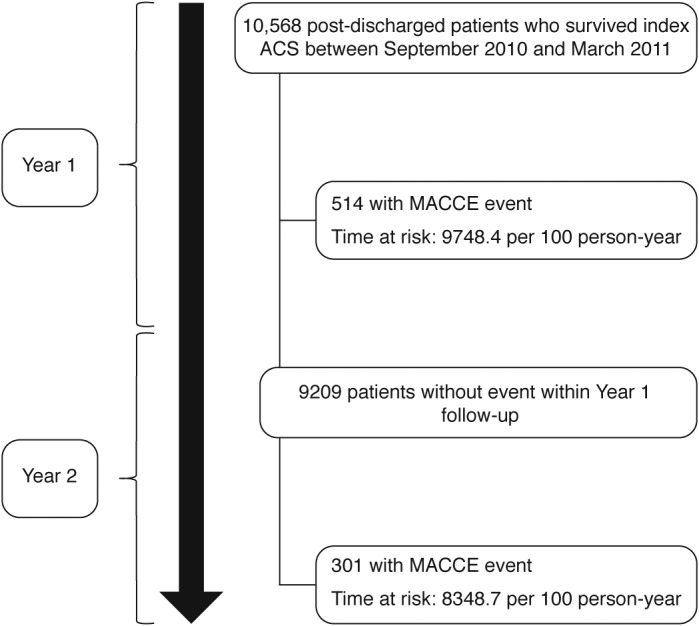
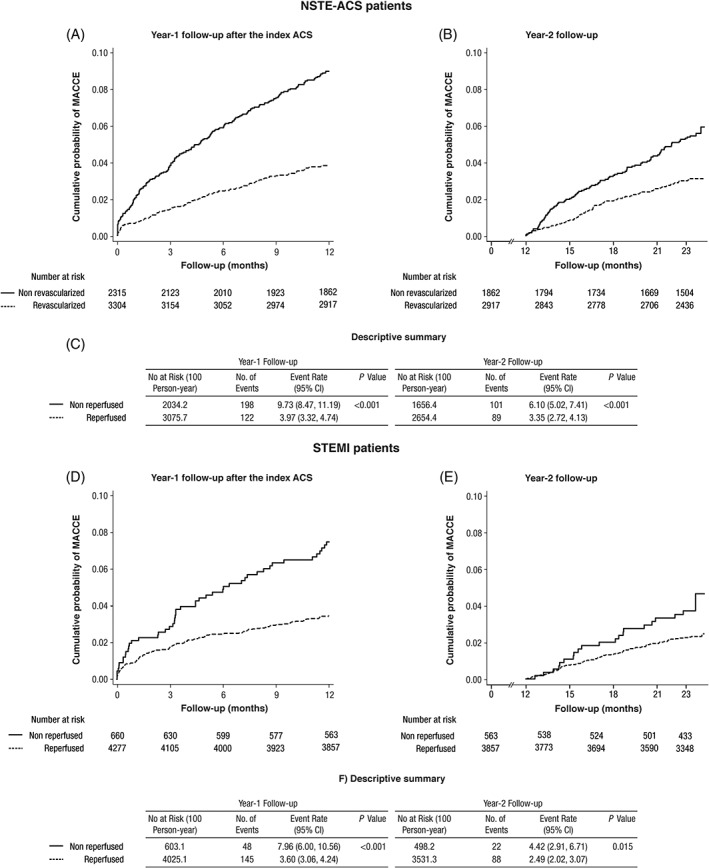
Methods: EPICOR (NCT01171404) was a prospective, international, real-world cohort study of consecutive patients hospitalized for ACS within 24 hours of symptom onset and surviving to discharge. Total of 10 568 patients were enrolled (555 hospitals; 20 countries) and followed-up for 2 years. From these, 4943 were admitted with ST-elevation myocardial infarction (STEMI) and 5625 with non-ST-elevation ACS (NSTE-ACS). Potential baseline predictors of major adverse cardiac and cerebrovascular events (MACCE; death, non-fatal myocardial infarction [MI], non-fatal stroke) were evaluated in year 1 and 2 post-discharge.
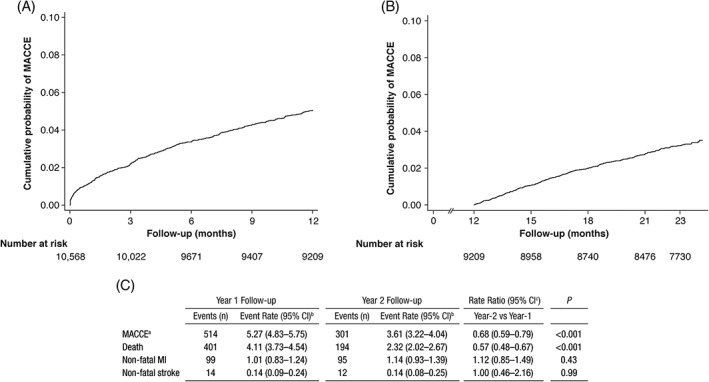
Results: MACCE incidence per 100 person-years at risk within and after 1 year was 5.3 vs 3.6, primarily death (4.1 vs 2.3), with no significant differences for MI or stroke. Older age, lack of coronary revascularization, raised creatinine, low hemoglobin, previous cardiac disease, previous chronic obstructive pulmonary disease, raised glucose, male sex, and geographic region were risk factors for MACCE in both year 1 and 2. By contrast, low ejection fraction, poorer quality of life, low body mass index (BMI) <20 kg/m2 , in-hospital cardiac complications, and Killip class lost predictive power after 1 year.
Conclusion: We observed continuous MACCE risk during 2 years of follow-up after discharge for ACS, with greater mortality within the first year. Specific predictors at discharge for events after 1 year could not be identified.
Keywords: acute coronary syndrome; hospital discharge; mortality; prognostic model; risk predictor.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
Xavier Rossello has nothing to disclose. Stuart J. Pocock has received research and statistical consulting honoraria from AstraZeneca. Héctor Bueno has received advisory/consulting fees from Abbott, AstraZeneca, Bayer, Bristol‐Myers Squibb, Daiichi‐Sankyo, Eli Lilly, Novartis, Pfizer, Sanofi, and Servier, and grants from AstraZeneca. Frans van de Werf has received consulting fees and research grants from Boehringer Ingelheim and Merck, and consulting fees from Roche, Sanofi‐Aventis, AstraZeneca, and The Medicines Company. Nicolas Danchin has received fees for lectures or consulting from Amgen, AstraZeneca, Bayer, Bristol‐Myers Squibb, Boehringer Ingelheim, Daiichi‐Sankyo, Eli‐Lilly, MSD, Novo‐Nordisk, Pfizer, Sanofi, and Servier, and research grants from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi‐Sankyo, Eli‐Lilly, Merck, Pfizer, and Sanofi. Lieven Annemans received honoraria from AstraZeneca, Bayer, and BMS. Jesús Medina is an employee of AstraZeneca. Uwe Zeymer has received honoraria from AstraZeneca, Bayer, BMS, Daiichi Sankyo, Eli Lilly, Pfizer, Novartis, Medicines Company, Sanofi, and Amgen.
Figures
References
-
- Rossello X, Pocock SJ, Julian DG. Long‐term use of cardiovascular drugs: challenges for research and for patient care. J Am Coll Cardiol. 2015;66:1273‐1285. - PubMed
-
- Setoguchi S, Glynn RJ, Avorn J, Mittleman MA, Levin R, Winkelmayer WC. Improvements in long‐term mortality after myocardial infarction and increased use of cardiovascular drugs after discharge: a 10‐year trend analysis. J Am Coll Cardiol. 2008;51:1247‐1254. - PubMed
-
- Jernberg T, Hasvold P, Henriksson M, Hjelm H, Thuresson M, Janzon M. Cardiovascular risk in post‐myocardial infarction patients: nationwide real world data demonstrate the importance of a long‐term perspective. Eur Heart J. 2015;36:1163‐1170. - PubMed
-
- Fox KAA, Carruthers KF, Dunbar DR, et al. Underestimated and under‐recognized: the late consequences of acute coronary syndrome (GRACE UK‐Belgian study). Eur Heart J. 2010;31:2755‐2764. - PubMed
-
- Eagle KA, Lim MJ, Dabbous OH, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6‐month postdischarge death in an international registry. JAMA. 2004;291:2727‐2733. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
