

Differential use of medical versus surgical androgen deprivation therapy for patients with metastatic prostate cancer
- PMID: 30444526
- PMCID: PMC6340740
- DOI: 10.1002/cncr.31826
Differential use of medical versus surgical androgen deprivation therapy for patients with metastatic prostate cancer
Abstract
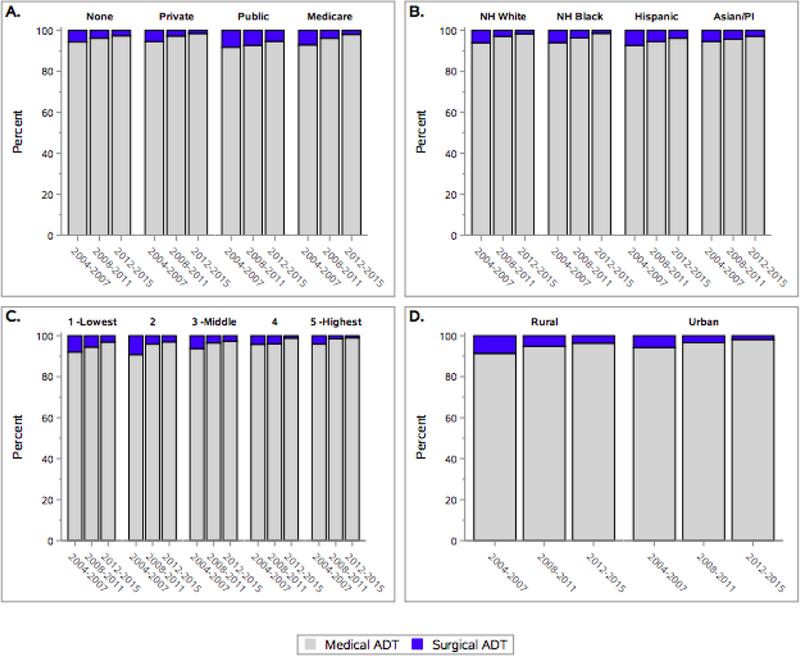
Background: Surgical and medical androgen deprivation therapy (ADT) strategies are comparable in their ability to suppress serum testosterone levels as treatment in patients with metastatic prostate cancer but differ with regard to cost and impact on quality of life. Medical ADT is associated with better long-term quality of life due to the flexibility of possible therapy interruption but comes with a higher cumulative cost. In the current study, the authors examined whether surgical ADT (ie, bilateral orchiectomy) was used differentially by race/ethnicity and other social factors.
Methods: The authors identified patients with metastatic disease at the time of diagnosis through the California Cancer Registry. The association between race/ethnicity and receipt of surgical ADT was modeled using multivariable Firth logistic regression adjusting for age, Gleason score, prostate-specific antigen level, clinical tumor and lymph node classification, neighborhood socioeconomic status (SES), insurance, marital status, comorbidities, initial treatment (radiotherapy, chemotherapy), location of care, rural/urban area of residence, and year of diagnosis.
Results: The authors examined a total of 10,675 patients with metastatic prostate cancer, 11.4% of whom were non-Hispanic black, 8.4% of whom were Asian/Pacific Islander, 18.5% of whom were Hispanic/Latino, and 60.5% of whom were non-Hispanic white. In the multivariable model, patients found to be more likely to receive surgical ADT were Hispanic/Latino (odds ratio [OR], 1.32; 95% confidence interval [95% CI], 1.01-1.72), were from a low neighborhood SES (OR, 1.96; 95% CI, 1.34-2.89) or rural area (OR, 1.49; 95% CI, 1.15-1.92), and had Medicaid/public insurance (OR, 2.21; 95% CI, 1.58-3.10). Patients with military/Veterans Affairs insurance were significantly less likely to receive surgical ADT compared with patients with private insurance (OR, 0.34; 95% CI, 0.13-0.88).
Conclusions: Race/ethnicity, neighborhood SES, and insurance status appear to be significantly associated with receipt of surgical ADT. Future research will need to characterize other differences in initial treatments among men with advanced prostate cancer based on race/ethnicity and aim to better understand what factors drive the association between surgical ADT among men of Hispanic origin or those from areas with low neighborhood SES.
Keywords: androgen deprivation therapy (ADT); cancer disparities; metastatic prostate cancer; orchiectomy.
© 2018 American Cancer Society.
Conflict of interest statement
Figures
References
-
- Sharifi N, Gulley JL, and Dahut WL, Androgen deprivation therapy for prostate cancer. JAMA, 2005. 294(2): p. 238–44. - PubMed
-
- Lee DJ, et al. , Recent Changes in Prostate Cancer Screening Practices and Epidemiology. J Urol, 2017. 198(6): p. 1230–1240. - PubMed
-
- Fizazi K, et al. , Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med, 2017. 377(4): p. 352–360. - PubMed
