

Tobacco Use Assessment and Treatment in Cancer Patients: A Scoping Review of Oncology Care Clinician Adherence to Clinical Practice Guidelines in the U.S
- PMID: 30446582
- PMCID: PMC6369951
- DOI: 10.1634/theoncologist.2018-0246
Tobacco Use Assessment and Treatment in Cancer Patients: A Scoping Review of Oncology Care Clinician Adherence to Clinical Practice Guidelines in the U.S
Abstract
Background: Smoking after a cancer diagnosis negatively impacts health outcomes; smoking cessation improves symptoms, side effects, and overall prognosis. The Public Health Service and major oncology organizations have established guidelines for tobacco use treatment among cancer patients, including clinician assessment of tobacco use at each visit. Oncology care clinicians (OCCs) play important roles in this process (noted as the 5As: Asking about tobacco use, Advising users to quit, Assessing willingness to quit, Assisting in quit attempts, and Arranging follow-up contact). However, OCCs may not be using the "teachable moments" related to cancer diagnosis, treatment, and survivorship to provide cessation interventions.
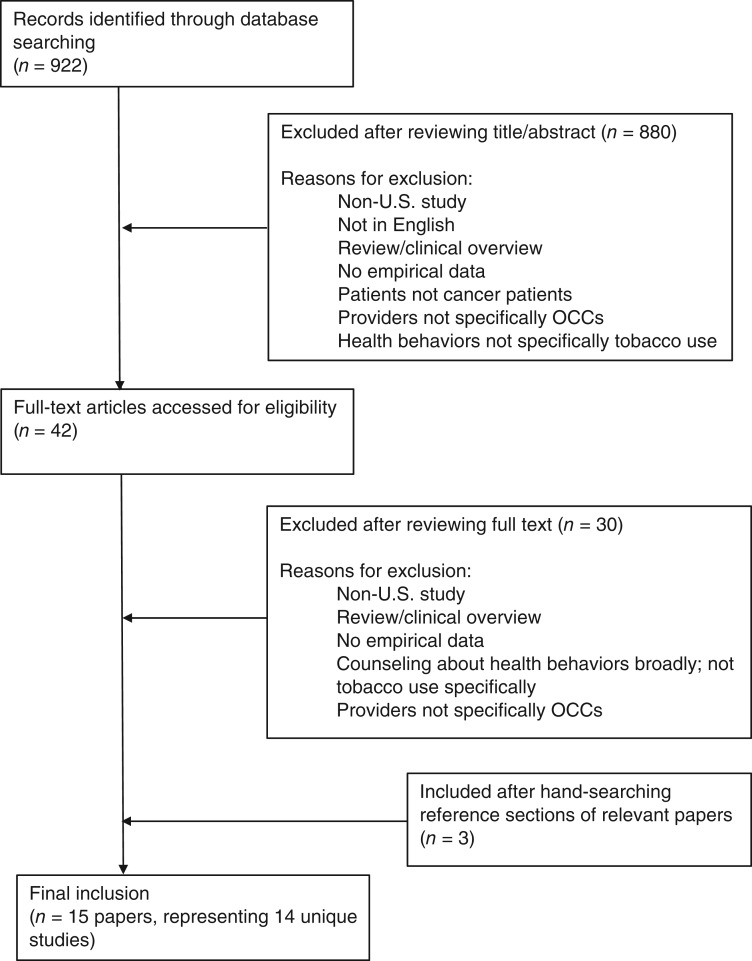
Materials and methods: In this scoping literature review of articles from 2006 to 2017, we discuss (1) frequency and quality of OCCs' tobacco use assessments with cancer patients and survivors; (2) barriers to providing tobacco treatment for cancer patients; and (3) the efficacy and future of provider-level interventions to facilitate adherence to tobacco treatment guidelines.
Results: OCCs are not adequately addressing smoking cessation with their patients. The reviewed studies indicate that although >75% assess tobacco use during an intake visit and >60% typically advise patients to quit, a substantially lower percentage recommend or arrange smoking cessation treatment or follow-up after a quit attempt. Less than 30% of OCCs report adequate training in cessation interventions.
Conclusion: Intervention trials focused on provider- and system-level change are needed to promote integration of evidence-based tobacco treatment into the oncology setting. Attention should be given to the barriers faced by OCCs when targeting interventions for the oncologic context.
Implications for practice: This article reviews the existing literature on the gap between best and current practices for tobacco use assessment and treatment in the oncologic context. It also identifies clinician- and system-level barriers that should be addressed in order to lessen this gap and provides suggestions that could be applied across different oncology practice settings to connect patients with tobacco use treatments that may improve overall survival and quality of life.
背景。癌症诊断后吸烟会对健康结果产生负面影响;而戒烟可以改善病症、副作用和整体预后。公共卫生部门和主要的肿瘤学组织已经确立了有关癌症患者戒烟治疗的指南,包括每次访视时对烟草使用情况进行临床评估。在这一过程(又称为 5A:询问 (Asking) 烟草使用情况;建议 (Advising) 使用者戒烟;评估 (Assessing) 戒烟意愿;协助 (Advising) 戒烟尝试;以及安排 (Arranging) 随访联系)中,肿瘤学保健医生 (OCC) 发挥着重要作用。然而,OCC 未必会利用这些与癌症诊断、治疗和存活率相关的“受教时刻”来提供戒烟干预。
材料和方法。在本篇囊括 2006 年至 2017 年多篇文章的范围文献综述中,我们讨论了 (1) OCC 对癌症患者和幸存者烟草使用情况评估的频率和质量;(2) 为癌症患者提供戒烟治疗的屏障;以及 (3) 提供者层面的干预对促进遵循戒烟指南的有效性和未来前景。
结果。OCC 没有充分解决患者的戒烟问题。回顾研究表明,尽管 75% 以上的患者在最初访视期间评估了烟草使用情况,并且 60% 以上的结果通常建议患者戒烟,但是在尝试戒烟后,建议或安排戒烟治疗或随访的百分比明显降低。只有不到 30% 的 OCC 报告提供了适当的戒烟干预培训。
结论。需要针对提供者层面和系统层面的变化进行干预试验,以促进在肿瘤学环境中纳入基于证据的戒烟治疗。在针对肿瘤学背景进行干预时,应注意 OCC 所面临的屏障。
实践意义:本文回顾了有关肿瘤学环境中烟草使用情况评估及戒烟治疗的最佳实践与现行实践之间差距的现有文献。同时确定了为缩小这种差距,应该解决的临床医生层面和系统层面的屏障,并提供了适用于不同肿瘤学实践环境的建议,以便将患者与戒烟治疗相关联,从而改善整体存活率和生活质量。
Keywords: Cancer; Oncologists; Patients; Smoking cessation; Tobacco.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
Comment in
-
Care for Smoking Cessation Must Be Proactive and Based on a Combination of Pharmacology and Psychology.Oncologist. 2019 Jul;24(7):e607. doi: 10.1634/theoncologist.2018-0817. Epub 2019 Mar 19. Oncologist. 2019. PMID: 30890625 Free PMC article.
References
-
- American Cancer Society . Cancer Facts & Figures 2016. Cancer Facts Fig 2016. 2016:1‐9. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts....
-
- US Department of Health and Human Services . The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention, 2014.
-
- Shields PG, Herbst RS, Arenberg D et al. Smoking Cessation, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2016;14:1430–1468. - PubMed
-
- Hanna N, Mulshine J, Wollins DS et al. Tobacco cessation and control a decade later: American Society of Clinical Oncology policy statement update. J Clin Oncol 2013;31:3147–3157. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
