

Inflammatory and coagulatory parameters linked to survival in critically ill children with sepsis
- PMID: 30446841
- PMCID: PMC6240023
- DOI: 10.1186/s13613-018-0457-8
Inflammatory and coagulatory parameters linked to survival in critically ill children with sepsis
Abstract
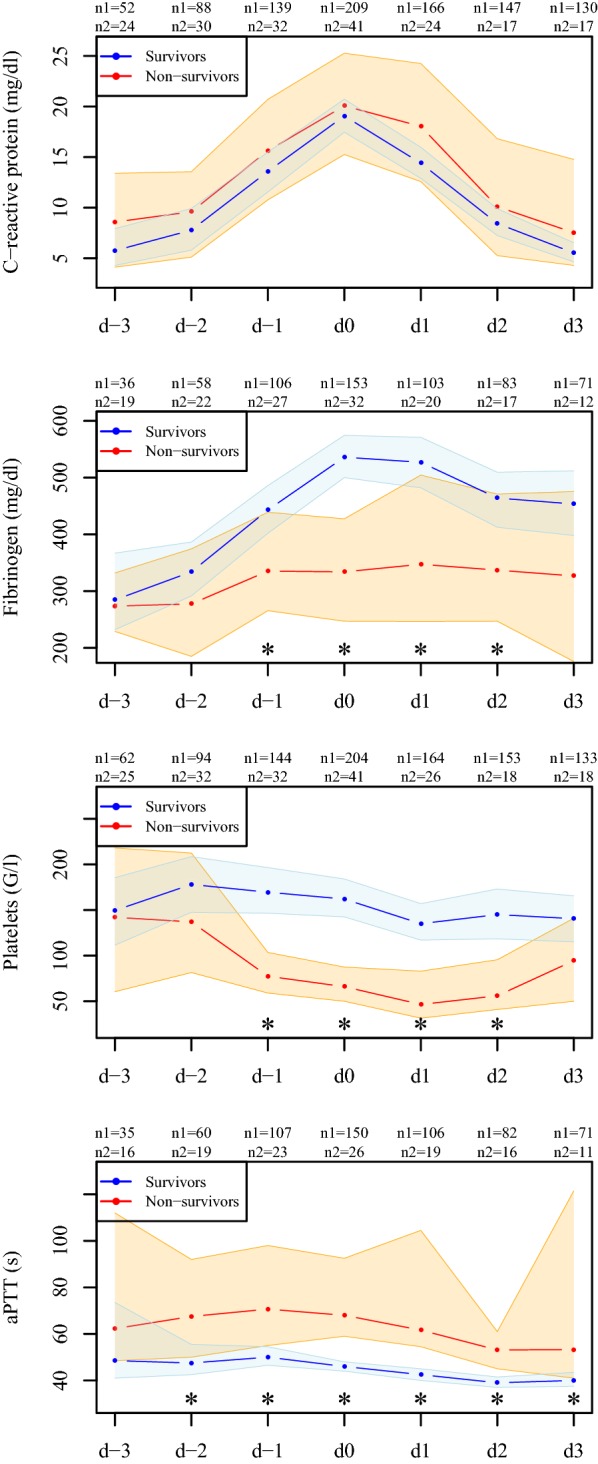
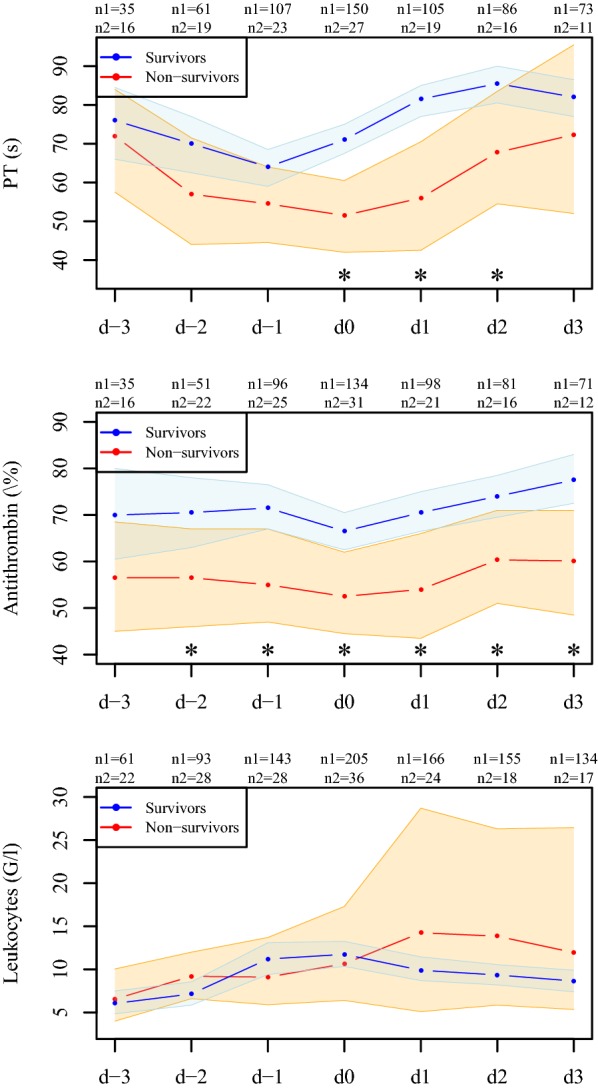
Background: Sepsis is associated with a deflection of inflammatory and coagulative parameters, since some clotting factors are known to be involved in the host's defense against infection and inflammation. These parameters could play a crucial role in the course of sepsis and be used as prognostic markers in critically ill children.
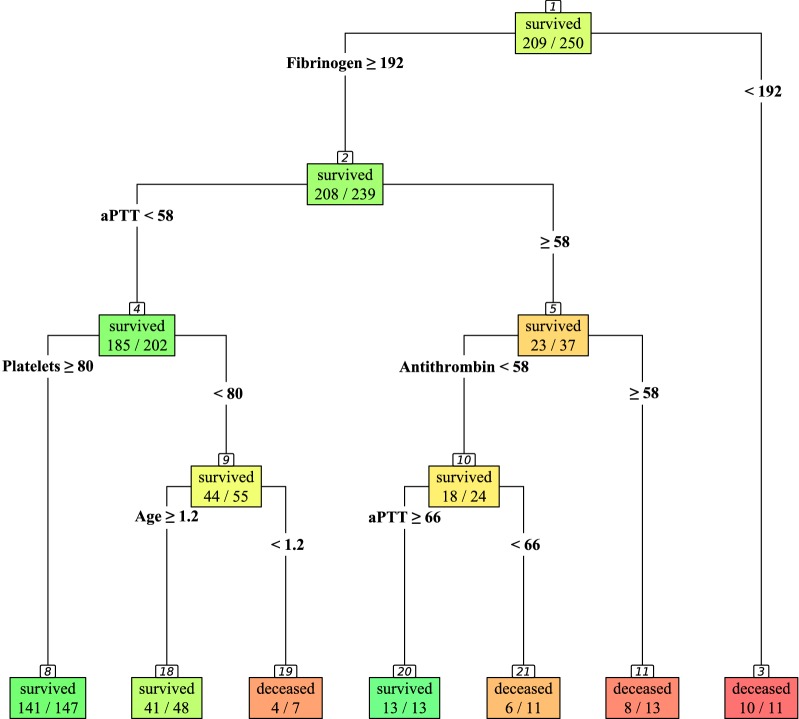
Methods: A total of 250 critically ill pediatric patients diagnosed with sepsis were retrospectively analyzed to identify routinely measured predictors for in-hospital mortality at the peak level of C-reactive protein. Those parameters entered multivariate logistic regression analysis as well as a decision tree for survival.
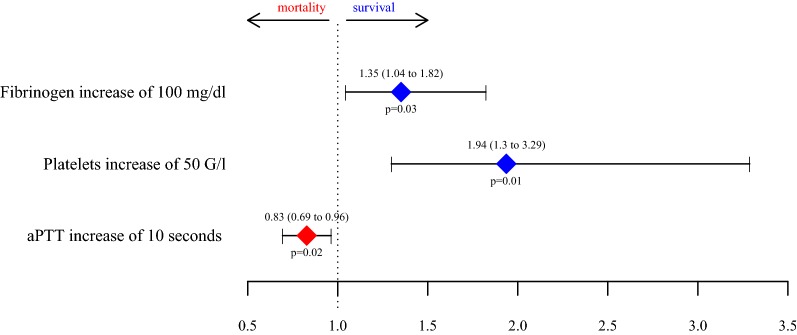
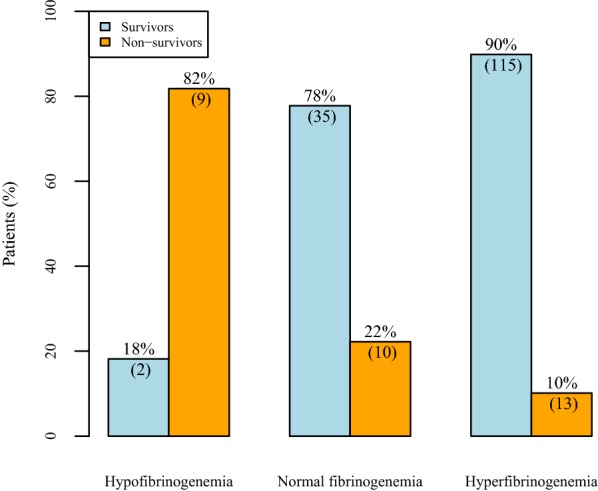
Results: Multivariate logistic regression analysis revealed fibrinogen, platelets and activated partial thromboplastin time (aPTT) at the peak level of C-reactive protein to be predictors for survival (p = 0.03, p = 0.01 and p = 0.02, respectively). An increase in fibrinogen and platelets is linked to survival, whereas an aPTT prolongation is associated with higher mortality; adjusted odds ratios (95% CI) for an increase of 100 mg/dl in fibrinogen are 1.35 (1.04-1.82) per 50 G/l platelets 1.94 (1.3-3.29) and 0.83 (0.69-0.96) for an aPTT prolongation of 10 s. Decision tree analysis shows that a fibrinogen level below 192 mg/dl (90.9% vs. 13% mortality) is most distinctive in non-survivors.
Conclusions: High levels of fibrinogen and platelets as well as a non-overshooting aPTT are associated with a higher survival rate in pediatric patients with diagnosed sepsis. In particular, hypofibrinogenemia is distinctive for a high mortality rate in septic critically ill children.
Keywords: Children; Coagulation; Fibrinogen; Inflammation; Platelets; Sepsis; Survival.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
