

Easily detected signs of perineural tumour spread in head and neck cancer
- PMID: 30446949
- PMCID: PMC6269343
- DOI: 10.1007/s13244-018-0672-8
Easily detected signs of perineural tumour spread in head and neck cancer
Abstract
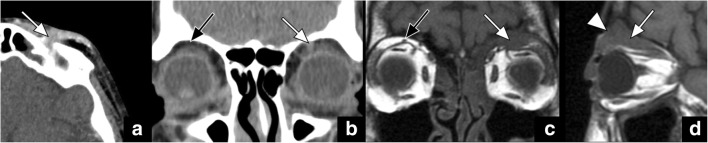
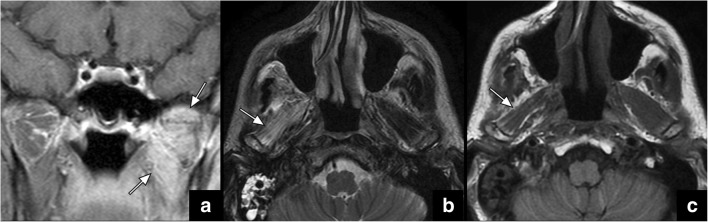
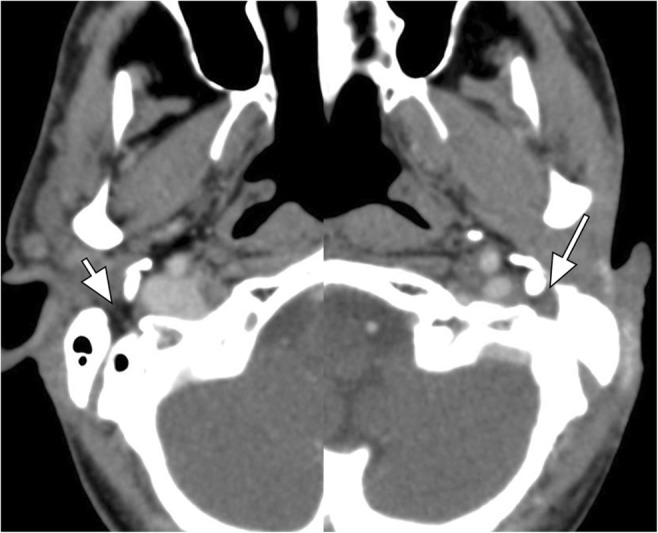
Perineural tumour spread (PNTS) in head and neck oncology is most often caused by squamous cell carcinoma. The most frequently affected nerves are the trigeminal and facial nerves. Up to 40% of patients with PNTS may be asymptomatic. Therefore, the index of suspicion should be high when evaluating imaging studies of patients with head and neck cancer. This review describes a "quick search checklist" of easily detected imaging signs of PNTS. TEACHING POINTS: • A distinctive feature of head and neck tumours is growth along nerves. • Perineural tumour spread is most often caused by squamous cell carcinoma. • There are several key findings for the detection of perineural tumour spread.
Keywords: Head and neck; Imaging; Oncology; Perineural tumour spread.
Conflict of interest statement
The authors have nothing to disclose.
Figures





References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2015) Global cancer statistics, 2012. CA Cancer J Clin 65:87–108 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
