

Challenges in assessing the sunscreen-melanoma association
- PMID: 30447006
- PMCID: PMC6451658
- DOI: 10.1002/ijc.31997
Challenges in assessing the sunscreen-melanoma association
Abstract
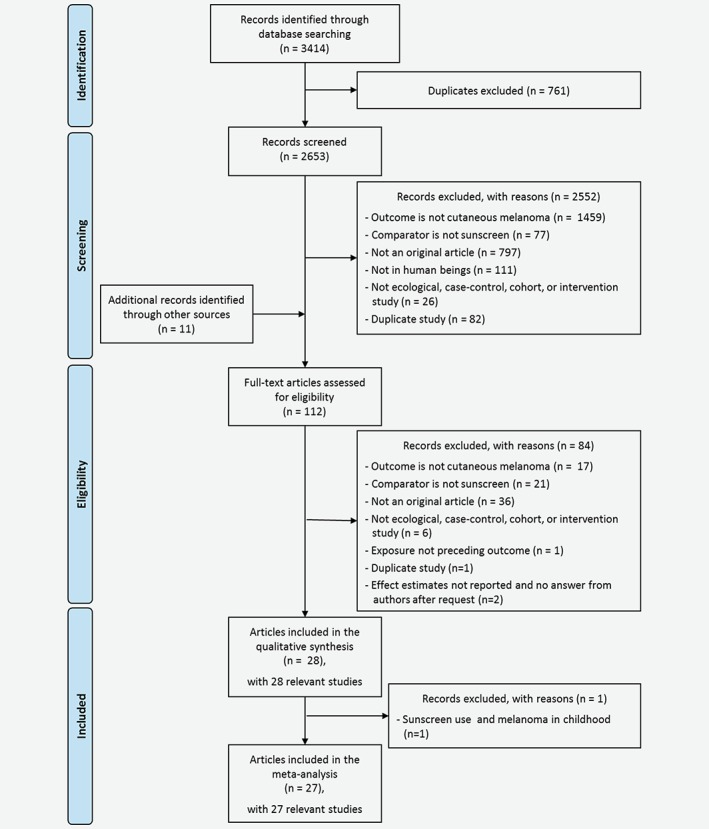
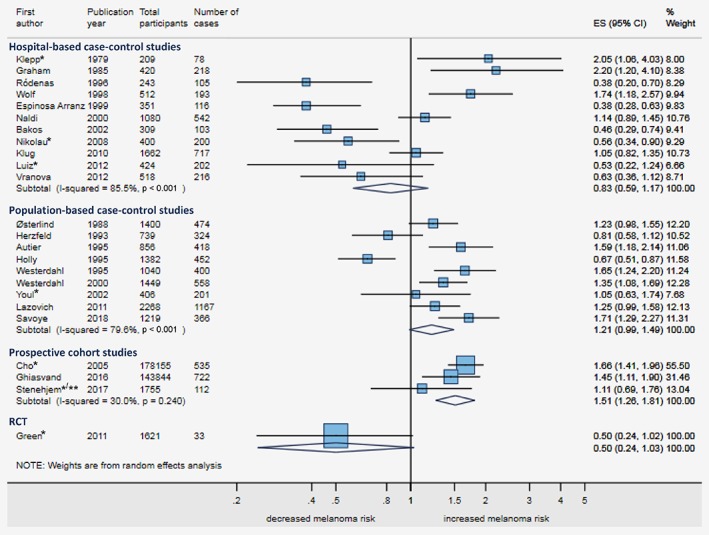
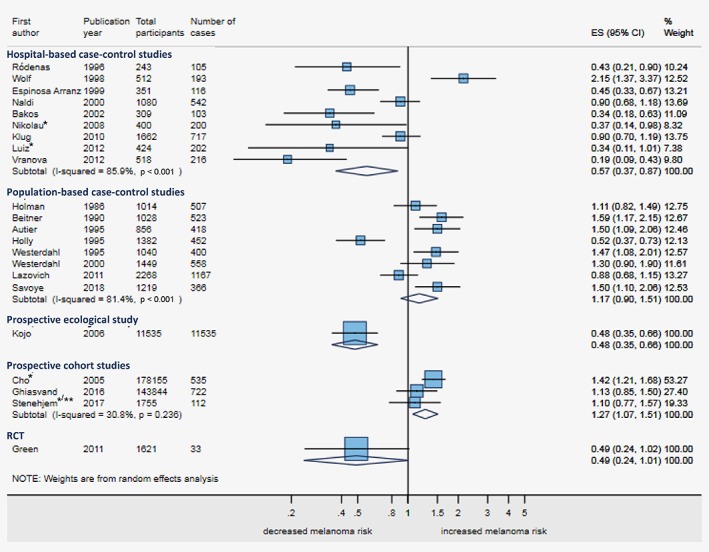
Whether sunscreen use affects melanoma risk has been widely studied with contradictory results. To answer this question we performed a systematic review of all published studies, accounting for sources of heterogeneity and bias. We searched for original articles investigating the sunscreen-melanoma association in humans to February 28, 2018. We then used random-effects meta-analysis to combine estimates of the association, stratified by study design. Stratified meta-analysis and meta-regression were used to identify sources of heterogeneity. We included 21,069 melanoma cases from 28 studies published 1979-2018: 23 case-control (11 hospital-based, 12 population-based), 1 ecological, 3 cohort and 1 randomised controlled trial (RCT). There was marked heterogeneity across study designs and among case-control studies but adjustment for confounding by sun exposure, sunburns and phenotype systematically moved estimates toward decreased melanoma risk among sunscreen users. Ever- vs. never-use of sunscreen was inversely associated with melanoma in hospital-based case-control studies (adjusted odds ratio (OR) = 0.57, 95%confidence interval (CI) 0.37-0.87, pheterogeneity < 0.001), the ecological study (rate ratio = 0.48, 95%CI 0.35-0.66), and the RCT (hazard ratio (HR) = 0.49, 95%CI 0.24-1.01). It was not associated in population-based case-control studies (OR = 1.17, 95%CI 0.90-1.51, pheterogeneity < 0.001) and was positively associated in the cohort studies (HR = 1.27, 95%CI 1.07-1.51, pheterogeneity = 0.236). The association differed by latitude (pinteraction = 0.042), region (pinteraction = 0.008), adjustment for naevi/freckling (pinteraction = 0.035), and proportion of never-sunscreen-users (pinteraction = 0·012). Evidence from observational studies on sunscreen use and melanoma risk was weak and heterogeneous, consistent with the challenges of controlling for innate confounding by indication. The only RCT showed a protective effect of sunscreen.
Keywords: melanoma; meta-analysis; skin cancer; sun protection; sunscreen.
© 2018 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Figures
Similar articles
-
Phenotypic markers, sunlight-related factors and sunscreen use in patients with cutaneous melanoma: an Austrian case-control study.Melanoma Res. 1998 Aug;8(4):370-8. doi: 10.1097/00008390-199808000-00012. Melanoma Res. 1998. PMID: 9764814
-
Melanoma risk in relation to use of sunscreen or other sun protection methods.Cancer Epidemiol Biomarkers Prev. 2011 Dec;20(12):2583-93. doi: 10.1158/1055-9965.EPI-11-0705. Epub 2011 Oct 20. Cancer Epidemiol Biomarkers Prev. 2011. PMID: 22016471 Free PMC article.
-
Cutaneous malignant melanoma, sun exposure, and sunscreen use: epidemiological evidence.Br J Dermatol. 2002 Apr;146 Suppl 61:24-30. doi: 10.1046/j.1365-2133.146.s61.9.x. Br J Dermatol. 2002. PMID: 11966729 Review.
-
Melanoma and sunscreen use: need for studies representative of actual behaviours.Melanoma Res. 1997 Aug;7 Suppl 2:S115-20. Melanoma Res. 1997. PMID: 9578426 Review.
-
Sunscreen use and the risk for melanoma: a quantitative review.Ann Intern Med. 2003 Dec 16;139(12):966-78. doi: 10.7326/0003-4819-139-12-200312160-00006. Ann Intern Med. 2003. PMID: 14678916
Cited by
-
Nuclear and Urinary Measurements Show the Efficacy of Sun-Protection Factor 50+ Sunscreen against DNA Photoproducts upon Real-Life Recreational Exposure.JID Innov. 2023 Aug 29;3(6):100227. doi: 10.1016/j.xjidi.2023.100227. eCollection 2023 Nov. JID Innov. 2023. PMID: 37886699 Free PMC article.
-
Art of prevention: The importance of melanoma surveillance.Int J Womens Dermatol. 2020 Feb 5;6(4):257-259. doi: 10.1016/j.ijwd.2020.01.003. eCollection 2020 Sep. Int J Womens Dermatol. 2020. PMID: 33015281 Free PMC article. Review. No abstract available.
-
Etiologies of Melanoma Development and Prevention Measures: A Review of the Current Evidence.Cancers (Basel). 2021 Sep 30;13(19):4914. doi: 10.3390/cancers13194914. Cancers (Basel). 2021. PMID: 34638397 Free PMC article. Review.
-
Towards a paradigm shift in environmental health decision-making: a case study of oxybenzone.Environ Health. 2022 Jan 8;21(1):6. doi: 10.1186/s12940-021-00806-y. Environ Health. 2022. PMID: 34998398 Free PMC article. Review.
-
Laboratory testing of sunscreens on the US market finds lower in vitro SPF values than on labels and even less UVA protection.Photodermatol Photoimmunol Photomed. 2022 May;38(3):224-232. doi: 10.1111/phpp.12738. Epub 2021 Oct 19. Photodermatol Photoimmunol Photomed. 2022. PMID: 34601762 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. Cancer incidence and mortality worldwide: IARC CancerBase no. 11 [internet]. Lyon, France: International Agency for Research on Cancer, 2012.
-
- American Cancer Society . Cancer Facts & Figures 2012. Atlanta, GA: American Cancer Society, 2012.
-
- SEER ‐ Surveillance . Epidemiology and end result program: turning cancer data into discovery: NCI ‐ National Cancer Institute, 2014; Available from https://seer.cancer.gov.
-
- Ossio R, Roldan‐Marin R, Martinez‐Said H, et al. Melanoma: a global perspective. Nat Rev Cancer 2017;17:393–4. - PubMed
