

Diagnostic Imaging and Management of Common Intra-articular and Peri-articular Soft Tissue Tumors and Tumorlike Conditions of the Knee
- PMID: 30449023
- PMCID: PMC6445722
- DOI: 10.1055/s-0038-1675609
Diagnostic Imaging and Management of Common Intra-articular and Peri-articular Soft Tissue Tumors and Tumorlike Conditions of the Knee
Abstract
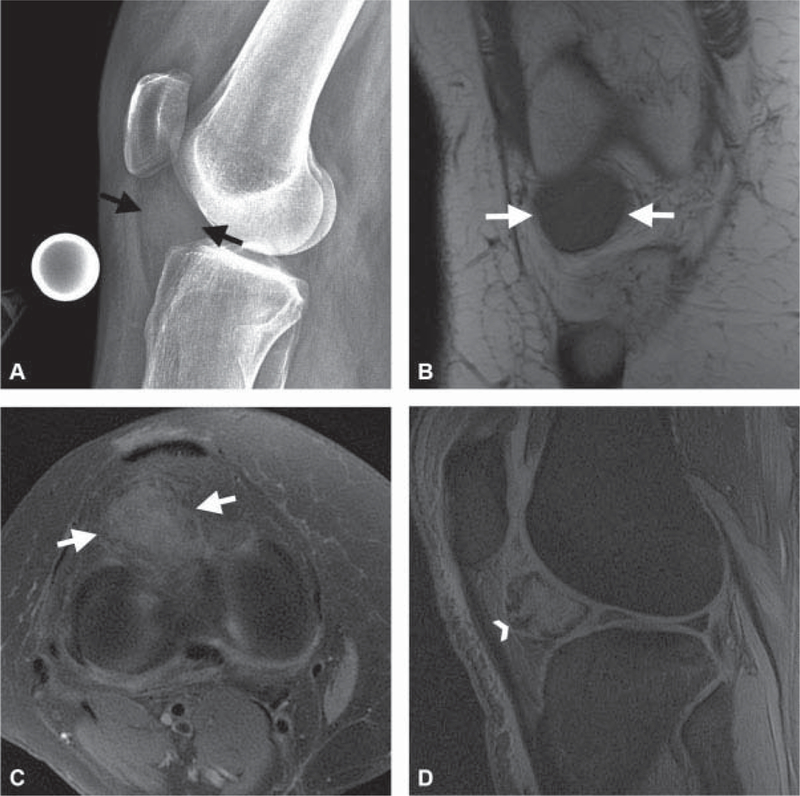
Intra-articular (IA) and peri-articular (PA) tumors of the knee are frequently encountered by orthopaedic surgeons. Nonetheless, due to the possibility of great morbidity and potential mortality, it is important to recognize and differentiate between benign and malignant lesions in a timely manner. Therefore, the purpose of this article is to provide a concise, practical, and updated review of commonly encountered IA and PA tumors including intratendinous gout, synovial chondromatosis, schwannoma, pigmented villonodular synovitis, and synovial sarcoma, and a detailed description of differentiating features to include various imaging modalities.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Conflict of interest statement
None.
Figures




References
-
- Smith E, Hoy DG, Cross M, et al. The global burden of other musculoskeletal disorders: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014;73(08):1462–1469 - PubMed
-
- Rodas G, Pedret C, Catala J, Soler R, Orozco L, Cusi M. Intratendi- nous gouty tophus mimics patellar tendonitis in an athlete. J Clin Ultrasound 2013;41(03):178–182 - PubMed
-
- Colberg RE, Henderson RG. Diagnosis and treatment of gouty tophi in the patellar tendon using ultrasound-guided needle barbotage: a case presentation. PM R 2017;9(09):938–942 - PubMed
