

Familial hypocalciuric hypercalcemia and related disorders
- PMID: 30449544
- PMCID: PMC6767927
- DOI: 10.1016/j.beem.2018.05.004
Familial hypocalciuric hypercalcemia and related disorders
Abstract
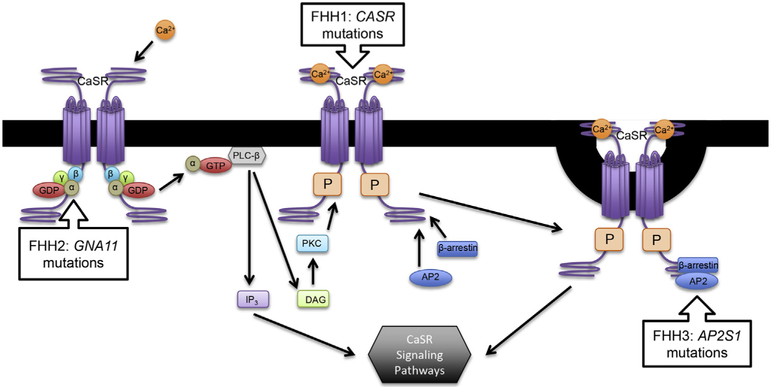
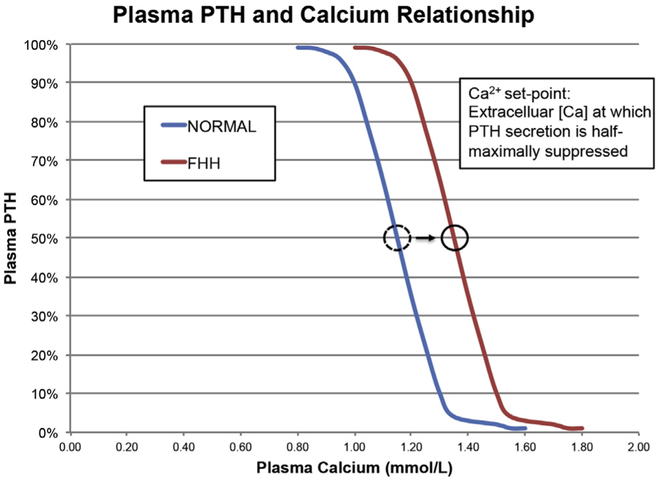
Familial hypocalciuric hypercalcemia (FHH) causes hypercalcemia by three genetic mechanisms: inactivating mutations in the calcium-sensing receptor, the G-protein subunit α11, or adaptor-related protein complex 2, sigma 1 subunit. While hypercalcemia in other conditions causes significant morbidity and mortality, FHH generally follows a benign course. Failure to diagnose FHH can result in unwarranted treatment or surgery for the mistaken diagnosis of primary hyperparathyroidism (PHPT), given the significant overlap of biochemical features. Determinations of urinary calcium excretion greatly aid in distinguishing PHPT from FHH, but overlap still exists in certain cases. It is important that 24-h urine calcium and creatinine be included in the initial workup of hypercalcemia. FHH should be considered if low or even low normal urinary calcium levels are found in what is typically an asymptomatic hypercalcemic patient. The calcimimetic cinacalcet has been used to treat hypercalcemia in certain symptomatic causes of FHH.
Keywords: Ca-sensing receptor; familial hypocalciuric hypercalcemia; hyperparathyroidism.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
References
-
- Wilhelm SM, Wang TS, Ruan DT, et al. The American association of endocrine surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg 2016;151:959–68. - PubMed
-
- Heath H 3rd, Hodgson SF, Kennedy MA. Primary hyperparathyroidism. Incidence, morbidity, and potential economic impact in a community. N Engl J Med 1980;302:189–93. - PubMed
-
- Foley TP Jr, Harrison HC, Arnaud CD, et al. Familial benign hypercalcemia. J Pediatr 1972;81:1060–7. - PubMed
