

Hyperammonemia in a Woman with Late-onset Ornithine Transcarbamylase Deficiency
- PMID: 30449781
- PMCID: PMC6478997
- DOI: 10.2169/internalmedicine.1851-18
Hyperammonemia in a Woman with Late-onset Ornithine Transcarbamylase Deficiency
Abstract
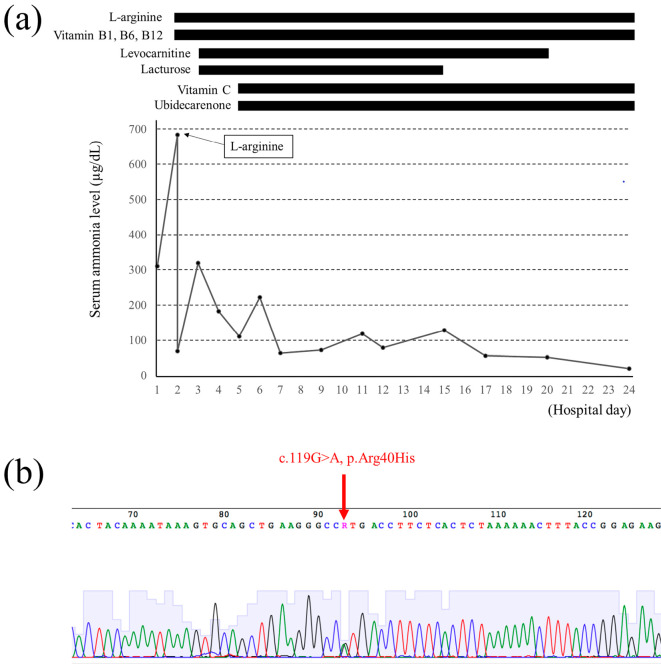
A 52-year-old woman developed vomiting and disturbance of consciousness after consuming raw fish and sushi on a trip. A blood test showed hyperammonemia (310 μg/dL) with a normal liver function. She fell into a deep coma, and her serum ammonia level increased to 684 μg/dL. L-arginine was administered as a diagnostic treatment for urea cycle disorder (UCD) and serum ammonia, and her consciousness levels improved. She was diagnosed with ornithine transcarbamylase deficiency (OTCD) by analyses of plasma amino acids, urinary orotic acid, and the OTC gene mutation. UCD should be considered for patients with hyperammonemia without severe liver function abnormalities.
Keywords: L-arginine; c.119G>A mutation; hyperammonemia; ornithine transcarbamylase deficiency; urea cycle; urea cycle disorder.
Conflict of interest statement
Figures
Similar articles
-
Hyperammonemia in a patient with late-onset ornithine carbamoyltransferase deficiency.J Korean Med Sci. 2012 May;27(5):556-9. doi: 10.3346/jkms.2012.27.5.556. Epub 2012 Apr 25. J Korean Med Sci. 2012. PMID: 22563224 Free PMC article.
-
Successful early management of a female patient with a metabolic stroke due to ornithine transcarbamylase deficiency.Pediatr Emerg Care. 2013 May;29(5):656-8. doi: 10.1097/PEC.0b013e31828ec2b9. Pediatr Emerg Care. 2013. PMID: 23640148
-
Late-onset ornithine transcarbamylase deficiency associated with hyperammonemia.Clin J Gastroenterol. 2017 Aug;10(4):383-387. doi: 10.1007/s12328-017-0753-0. Epub 2017 Jun 9. Clin J Gastroenterol. 2017. PMID: 28597413
-
[Hyperammonemia type II as an example of urea cycle disorder].Wiad Lek. 2006;59(7-8):512-5. Wiad Lek. 2006. PMID: 17209350 Review. Polish.
-
[Consensus on diagnosis and treatment of ornithine trans-carbamylase deficiency].Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020 Oct 25;49(5):539-547. doi: 10.3785/j.issn.1008-9292.2020.04.11. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020. PMID: 33210478 Free PMC article. Review. Chinese.
Cited by
-
Non-producer multiple myeloma presenting with acute hyperammonemic encephalopathy: case report.Diagn Pathol. 2023 Jan 4;18(1):1. doi: 10.1186/s13000-022-01285-6. Diagn Pathol. 2023. PMID: 36597112 Free PMC article.
-
Management of late onset urea cycle disorders-a remaining challenge for the intensivist?Ann Intensive Care. 2021 Jan 6;11(1):2. doi: 10.1186/s13613-020-00797-y. Ann Intensive Care. 2021. PMID: 33409766 Free PMC article. Review.
-
Psychological Stress Triggers a Hyperammonemia Episode in Patient with Ornithine Transcarbamylase Deficiency.Int J Environ Res Public Health. 2022 Sep 13;19(18):11516. doi: 10.3390/ijerph191811516. Int J Environ Res Public Health. 2022. PMID: 36141788 Free PMC article.
-
Common polymorphic OTC variants can act as genetic modifiers of enzymatic activity.Hum Mutat. 2021 Aug;42(8):978-989. doi: 10.1002/humu.24221. Epub 2021 Jun 3. Hum Mutat. 2021. PMID: 34015158 Free PMC article.
-
Corticosteroid suppresses urea-cycle-related gene expressions in ornithine transcarbamylase deficiency.BMC Gastroenterol. 2022 Mar 28;22(1):144. doi: 10.1186/s12876-022-02213-0. BMC Gastroenterol. 2022. PMID: 35346058 Free PMC article.
References
-
- Walker V. Ammonia toxicity and its prevention in inherited defects of the urea cycle. Diabetes Obes Metab 11: 823-835, 2009. - PubMed
-
- Walker V. Severe hyperammonemia in adults not explained by liver disease. Ann Clin Biochem 49: 1-15, 2012. - PubMed
-
- Treem WR. Inherited and acquired syndromes of hyperammonemia and encephalopathy in children. Semin Liver Dis 14: 236-258, 1994. - PubMed
-
- De Jonghe B, Janier V, Abderrahim N, Hillion D, Lacherade JC, Outin H. Urinary tract infection and coma. Lancet 360: 996, 2002. - PubMed
-
- Lora-Tamayo J, Palom X, Sarrá J, et al. . Multiple myeloma and hyperammonemic encephalopathy: review of 27 cases. Clin Lymphoma Myeloma 8: 363-369, 2008. - PubMed