

Update on the management of malignant peritoneal mesothelioma
- PMID: 30450299
- PMCID: PMC6204413
- DOI: 10.21037/tlcr.2018.08.03
Update on the management of malignant peritoneal mesothelioma
Abstract
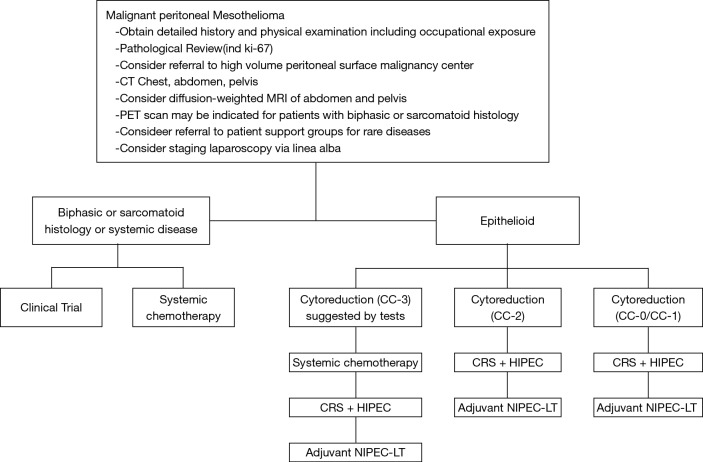
Malignant peritoneal mesothelioma (MPM) is a rare disease whose natural history is confined to the peritoneal space. Systemic chemotherapy has little impact on survival of patients with MPM. A surgical procedure with a goal of resection of all visible evidence of disease, called cytoreductive surgery (CRS) has been utilized in MPM patients. Also, regional chemotherapy with hyperthermic intraperitoneal chemotherapy (HIPEC) and normothermic intraperitoneal chemotherapy long-term (NIPEC-LT) have been effectively utilized in MPM patients. In the absence of CRS and HIPEC the median survival of MPM patients is approximately 1 year. The aggressive surgical approach plus regional chemotherapy has increased the median survival to more than 5 years. With NIPEC-LT added on, 70% 5-year survival has been reported. Knowledgeable patient selection for treatment is mandatory. The use of CRS, HIPEC and NIPEC-LT has greatly benefited patients with MPM. Global application of these treatments is indicated.
Keywords: Epithelial peritoneal mesothelioma; cisplatin; cytoreductive surgery (CRS); doxorubicin; early postoperative intraperitoneal chemotherapy (EPIC); hyperthermic perioperative chemotherapy (HIPEC); ifosfamide; normothermic intraperitoneal chemotherapy (NIPEC); paclitaxel.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources