Combination therapy for ischemic stroke: Novel approaches to lengthen therapeutic window of tissue plasminogen activator
- PMID: 30450415
- PMCID: PMC6187940
- DOI: 10.4103/bc.bc_21_18
Combination therapy for ischemic stroke: Novel approaches to lengthen therapeutic window of tissue plasminogen activator
Abstract
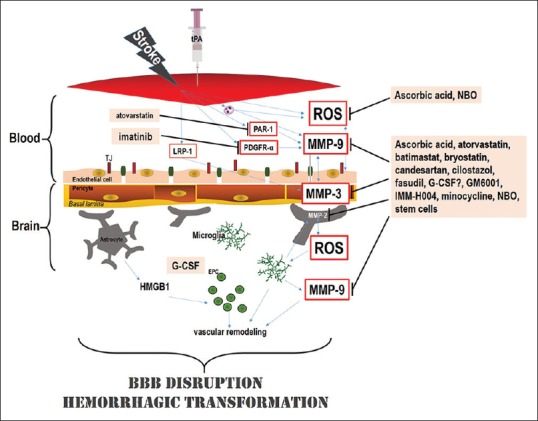
Tissue plasminogen activator (tPA) thrombolysis continues to be the gold standard therapy for ischemic stroke. Due to the time-limited treatment window, within 4.5 h of stroke onset, and a variety of potentially deadly complications related to delayed administration, particularly hemorrhagic transformation (HT), clinical use of tPA is limited. Combination therapies with other interventions, drug or nondrug, have been hypothesized as a logical approach to enhancing tPA effectiveness. Here, we discuss various potential pharmacological and nondrug treatments to minimize adverse effects, primarily HT, associated with delayed tPA administration. Pharmacological interventions include many that support the integrity of the blood-brain barrier (i.e., atorvastatin, batimastat, candesartan, cilostazol, fasudil, and minocycline), promote vascularization and preserve cerebrovasculature (i.e., coumarin derivative IMM-H004 and granulocyte-colony stimulating factor), employing other mechanisms of action (i.e., oxygen transporters and ascorbic acid). Nondrug treatments are comprised of stem cell transplantation and gas therapies with multi-faceted approaches. Combination therapy with tPA and the aforementioned treatments demonstrated promise for mitigating the adverse complications associated with delayed tPA treatment and rescuing stroke-induced behavioral deficits. Therefore, the conjunctive therapy method is a novel therapeutic approach that can attempt to minimize the limitations of tPA treatment and possibly increase the therapeutic window for ischemic stroke treatment.
Keywords: Blood–brain barrier; hemorrhage; matrix metalloproteinase; stem cell; tissue plasminogen activator.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Koton S, Schneider AL, Rosamond WD, Shahar E, Sang Y, Gottesman RF, et al. Stroke incidence and mortality trends in US communities, 1987 to 2011. JAMA. 2014;312:259–68. - PubMed
-
- Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. The NINDS t-PA stroke study group. Stroke. 1997;28:2109–18. - PubMed
-
- Graham GD. Tissue plasminogen activator for acute ischemic stroke in clinical practice: A meta-analysis of safety data. Stroke. 2003;34:2847–50. - PubMed
-
- Yip TR, Demaerschalk BM. Estimated cost savings of increased use of intravenous tissue plasminogen activator for acute ischemic stroke in Canada. Stroke. 2007;38:1952–5. - PubMed