

Secondary Oxalate Nephropathy: A Systematic Review
- PMID: 30450463
- PMCID: PMC6224620
- DOI: 10.1016/j.ekir.2018.07.020
Secondary Oxalate Nephropathy: A Systematic Review
Abstract
Introduction: Little is known of the clinical outcomes of secondary oxalate nephropathy. To inform clinical practice, we performed a systematic review of case reports and case series to examine the clinical characteristics and outcomes of patients with secondary oxalate nephropathy.
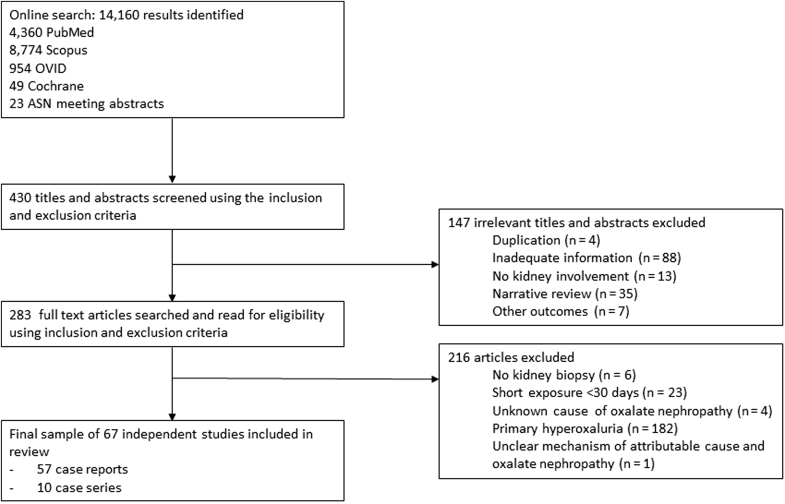
Methods: Electronic databases were searched for case reports and case series of individual cases or cohorts of patients with biopsy-proven oxalate nephropathy in native or transplanted kidneys from 1950 until January 2018.
Results: Fifty-seven case reports and 10 case series met the inclusion criteria, totaling 108 patients. The case series were meta-analyzed. Mean age was 56.4 years old, 59% were men, and 15% were kidney transplant recipients. Fat malabsorption (88%) was the most commonly attributed cause of oxalate nephropathy, followed by excessive dietary oxalate consumption (20%). The mean baseline serum creatinine was 1.3 mg/dl and peaked at 4.6 mg/dl. Proteinuria, hematuria, and urinary crystals was reported in 69%, 32%, and 26% of patients, respectively. Mean 24-hour urinary oxalate excretion was 85.4 mg/d. In addition to universal oxalate crystal deposition in tubules and/or interstitium, kidney biopsy findings included acute tubular injury (71%), tubular damage and atrophy (69%), and interstitial mononuclear cell infiltration (72%); 55% of patients required dialysis. None had complete recovery, 42% had partial recovery, and 58% remained dialysis-dependent. Thirty-three percent of patients died.
Conclusion: Secondary oxalate nephropathy is a rare but potentially devastating condition. Renal replacement therapy is required in >50% of patients, and most patients remain dialysis-dependent. Studies are needed for effective preventive and treatment strategies in high-risk patients with hyperoxaluria-enabling conditions.
Keywords: acute kidney injury; chronic kidney disease; nephrolithiasis; oxalate nephropathy; oxalosis; secondary oxalosis.
Figures
References
-
- Troxell M.L., Houghton D.C., Hawkey M. Enteric oxalate nephropathy in the renal allograft: an underrecognized complication of bariatric surgery. Am J Transplant. 2013;13:501–509. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
