

Diabetic macular edema: Evidence-based management
- PMID: 30451174
- PMCID: PMC6256891
- DOI: 10.4103/ijo.IJO_1240_18
Diabetic macular edema: Evidence-based management
Abstract
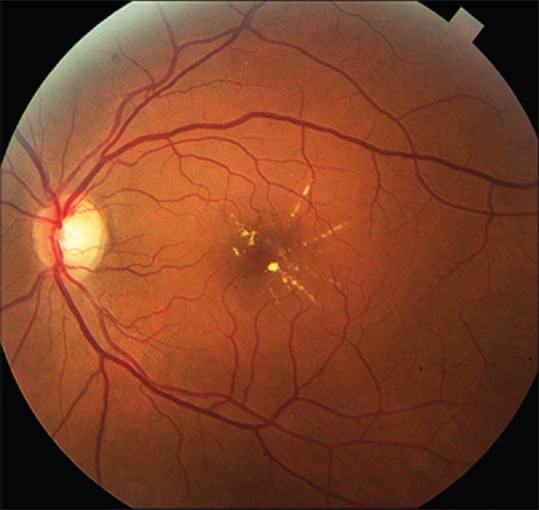
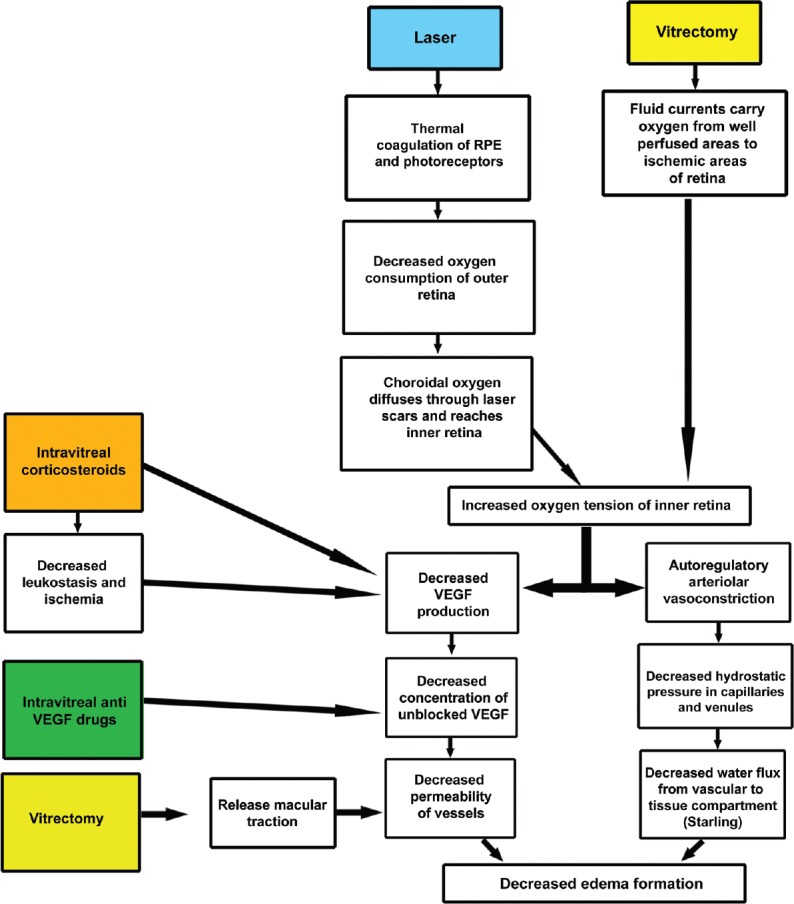
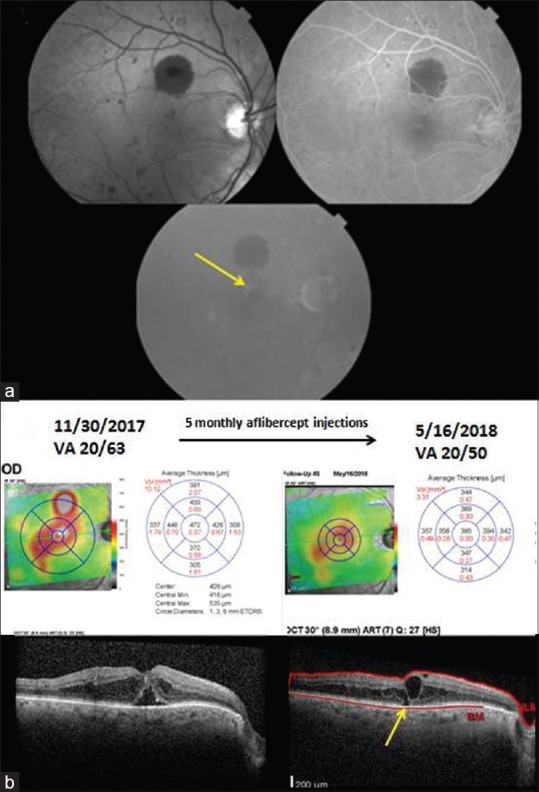
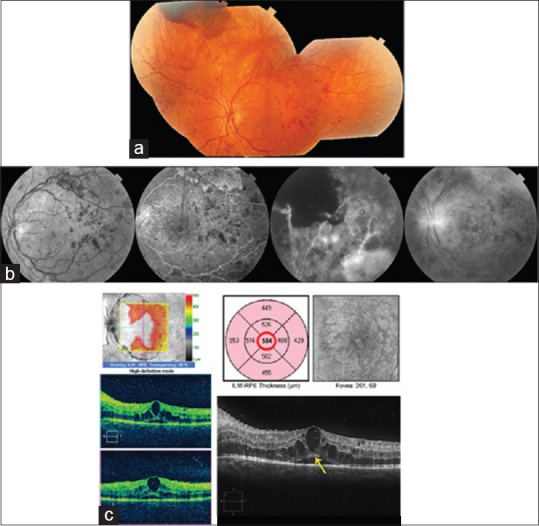
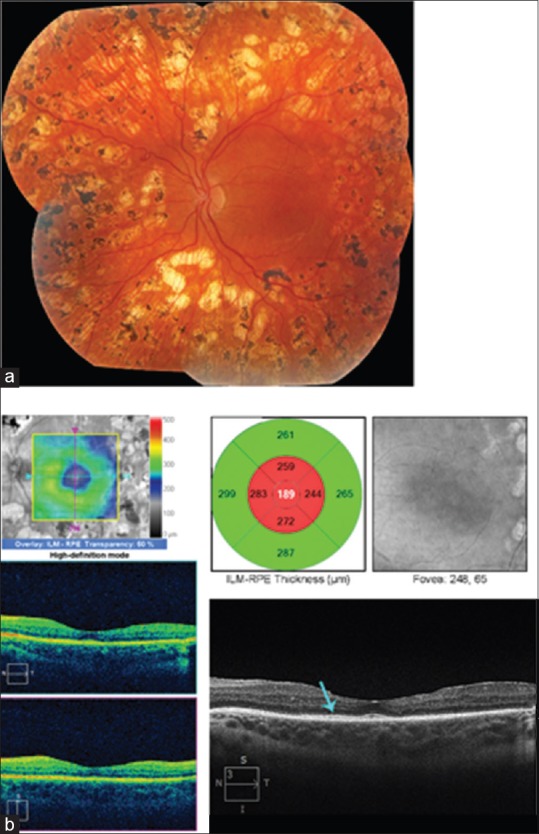
Diabetic macular edema (DME) is the most common cause of vision loss in patients with diabetic retinopathy with an increasing prevalence tied to the global epidemic in type 2 diabetes mellitus. Its pathophysiology starts with decreased retinal oxygen tension that manifests as retinal capillary hyperpermeability and increased intravascular pressure mediated by vascular endothelial growth factor (VEGF) upregulation and retinal vascular autoregulation, respectively. Spectral domain optical coherence tomography (SD-OCT) is the cornerstone of clinical assessment of DME. The foundation of treatment is metabolic control of hyperglycemia and blood pressure. Specific ophthalmic treatments include intravitreal anti-VEGF drug injections, intravitreal corticosteroid injections, focal laser photocoagulation, and vitrectomy, but a substantial fraction of eyes respond incompletely to all of these modalities resulting in visual loss and disordered retinal structure and vasculature visible on SD-OCT and OCT angiography. Efforts to close the gap between the results of interventions within randomized clinical trials and in real-world contexts, and to reduce the cost of care increasingly occupy innovation in the social organization of ophthalmic care of DME. Pharmacologic research is exploring other biochemical pathways involved in retinal vascular homeostasis that may provide new points of intervention effective in those cases unresponsive to current treatments.
Keywords: Diabetes; diabetic retinopathy; macular edema.
Conflict of interest statement
There are no conflicts of interest
Figures
References
-
- Klein R, Klein BE, Moss SE, Cruickshanks KJ. The Wisconsin epidemiologic study of diabetic retinopathy. XV. The long-term incidence of macular edema. Ophthalmology. 1995;102:7–16. - PubMed
-
- Klein R, Klein BE, Moss SE, Linton KL. The beaver dam eye study. Retinopathy in adults with newly discovered and previously diagnosed diabetes mellitus. Ophthalmology. 1992;99:58–62. - PubMed
-
- Klein R, Moss SE, Klein BE, Davis MD, DeMets DL. The Wisconsin epidemiologic study of diabetic retinopathy. XI. The incidence of macular edema. Ophthalmology. 1989;96:1501–10. - PubMed
-
- Xie XW, Xu L, Wang YX, Jonas JB. Prevalence and associated factors of diabetic retinopathy. The Beijing eye study 2006. Graefes Arch Clin Exp Ophthalmol. 2008;246:1519–26. - PubMed
-
- Rubino A, Rousculp MD, Davis K, Wang J, Girach A. Diagnosed diabetic retinopathy in France, Italy, Spain, and the United Kingdom. Prim Care Diabetes. 2007;1:75–80. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
