

Current management of diabetic tractional retinal detachments
- PMID: 30451175
- PMCID: PMC6256889
- DOI: 10.4103/ijo.IJO_1217_18
Current management of diabetic tractional retinal detachments
Abstract
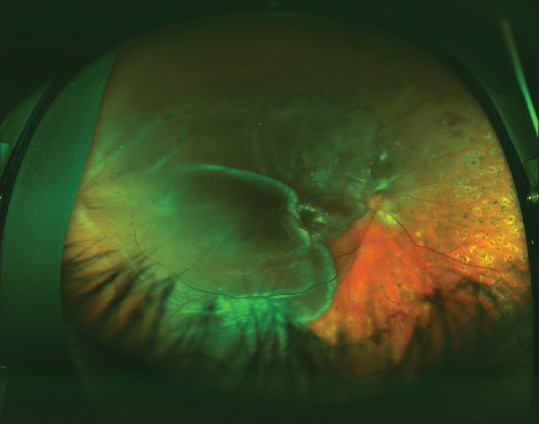
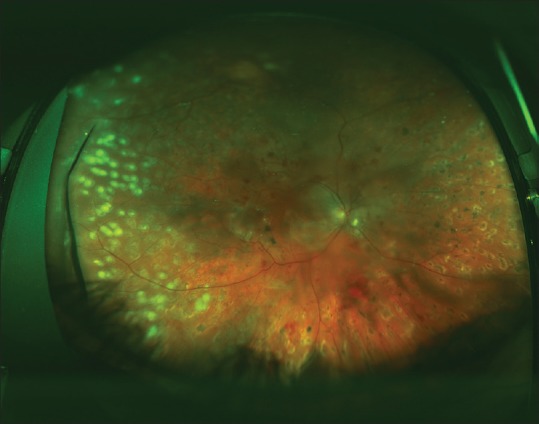
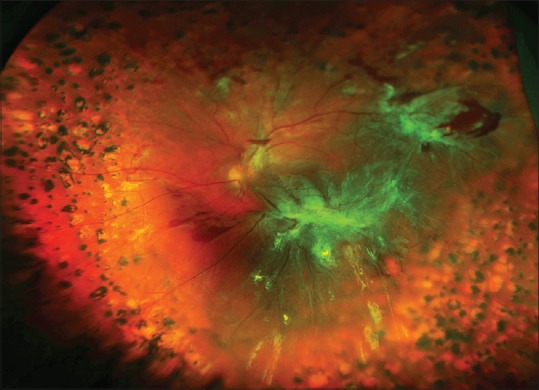
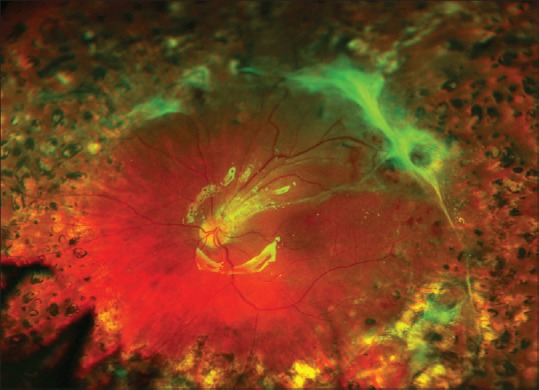
Twenty-five percent of diabetes-related vision loss stems from complications of proliferative diabetic retinopathy (PDR). Panretinal photocoagulation has been the preferred treatment of high-risk PDR for decades and more recently intravitreal injections of drugs that inhibit the actions of vascular endothelial growth factor have become popular. But despite these treatments PDR may progress uncontrollably to advanced pathologies such as traction retinal detachments (TRDs), combined traction/rhegmatogenous retinal detachments (TRD/RRDs), vitreous hemorrhages, rubeosis iridis, and traction maculopathies, which produce mild-to-severe loss of vision. TDR have long been the most common indication for PDR-related vitreoretinal surgery. Vitrectomy surgery is indicated for recent (<6 months duration) TRD involving the macula, progressive TRD that threatens the macula, and recent data suggest that chronic macula-involving TRDs (>6 months duration) may also benefit. Combined TRD/RRD represents a particularly challenging surgical condition but advances in surgical instrumentation, dissection techniques, and post-operative tamponade have produced excellent success rates. The recent development of small-gauge vitrectomy systems has persuaded most surgeons to switch platforms since these appear to produce shorter surgical times and quicker post-operative recoveries. Pre-operative injections of bevacizumab are frequently administered for persistent neovascularization to facilitate surgical dissection of pre-retinal fibrosis and reduce the incidence of post-operative hemorrhages. Recent trends toward earlier surgical intervention and expanded indications are likely to continue as surgical instrumentation and techniques are further developed.
Keywords: Diabetes; diabetic retinopathy; tractional retinal detachment; vitrectomy.
Conflict of interest statement
There are no conflicts of interest
Figures
References
-
- Kempen JH, O’Colmain BJ, Leske MC, Haffner SM, Klein R, Moss SE, et al. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004;122:552–63. - PubMed
-
- Centers for Disease Control and Prevention. Blindness caused by diabetes – massachusetts, 1987-1994. MMWR Morb Mortal Wkly Rep. 1996;45:937–41. - PubMed
-
- Photocoagulation for diabetic macular edema. Early treatment diabetic retinopathy study report number 1. Early treatment diabetic retinopathy study research group. Arch Ophthalmol. 1985;103:1796–806. - PubMed
-
- Boyer DS, Yoon YH, Belfort R, Jr, Bandello F, Maturi RK, Augustin AJ. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121:1904–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
