

Morphologic Overlap Between Inflammatory Myofibroblastic Tumor and IgG4-related Disease: Lessons From Next-generation Sequencing
- PMID: 30451733
- PMCID: PMC6637760
- DOI: 10.1097/PAS.0000000000001167
Morphologic Overlap Between Inflammatory Myofibroblastic Tumor and IgG4-related Disease: Lessons From Next-generation Sequencing
Abstract
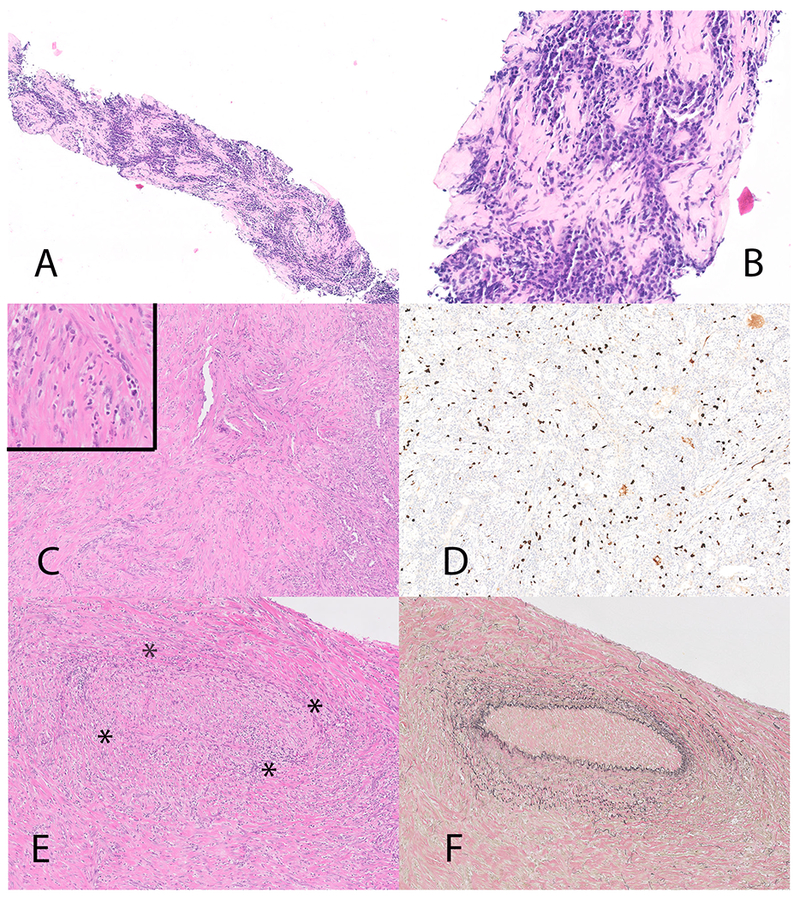
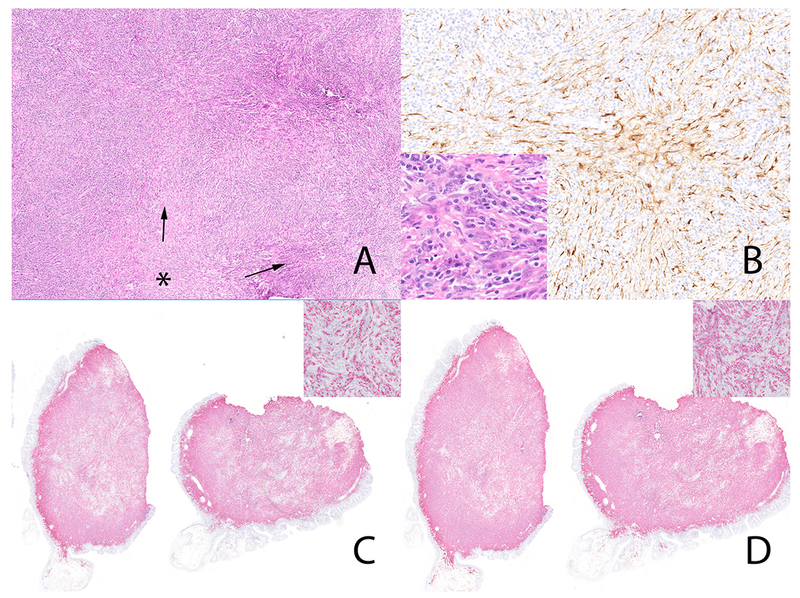
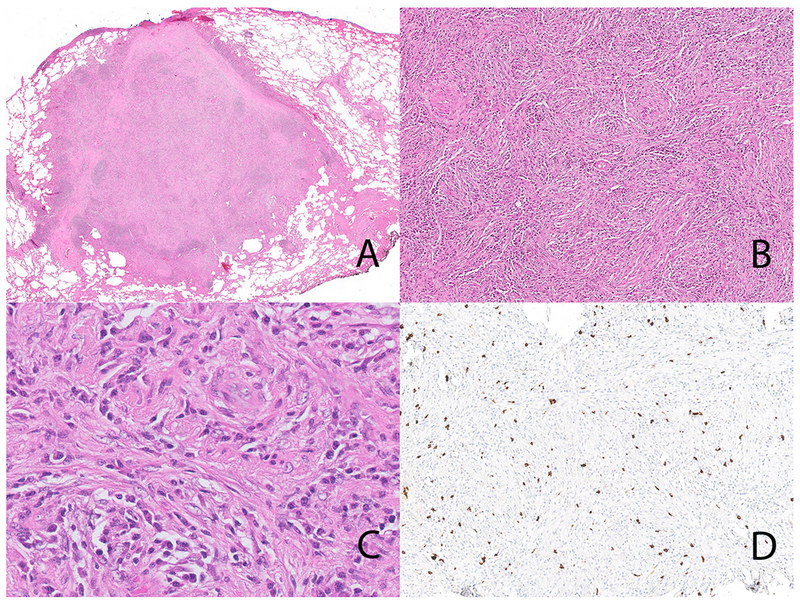
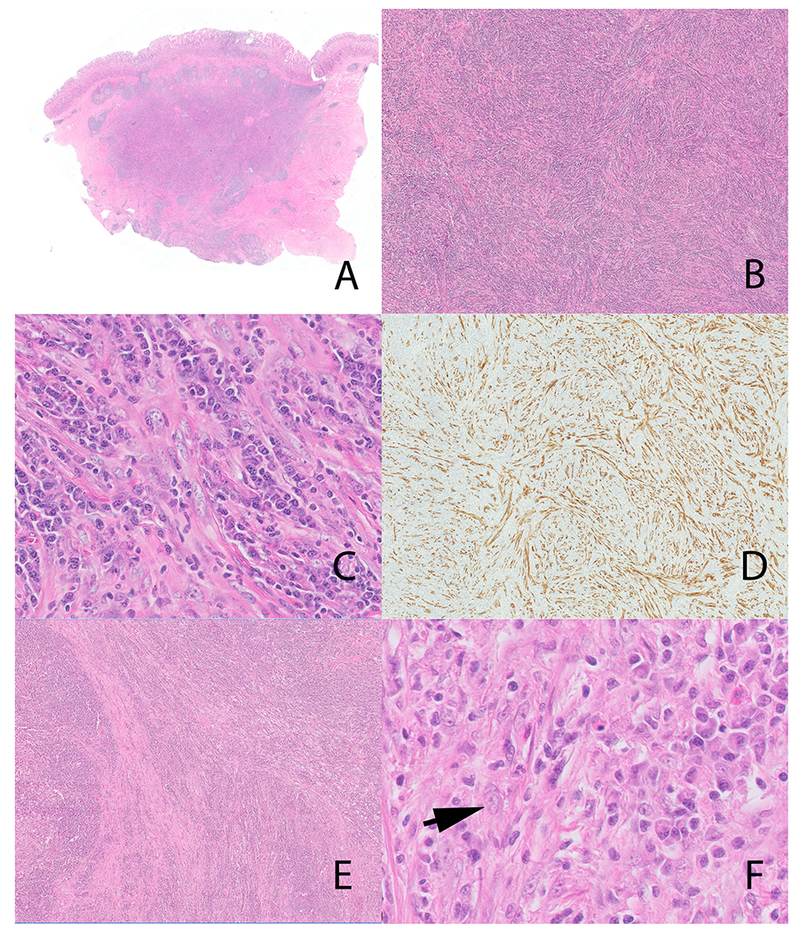
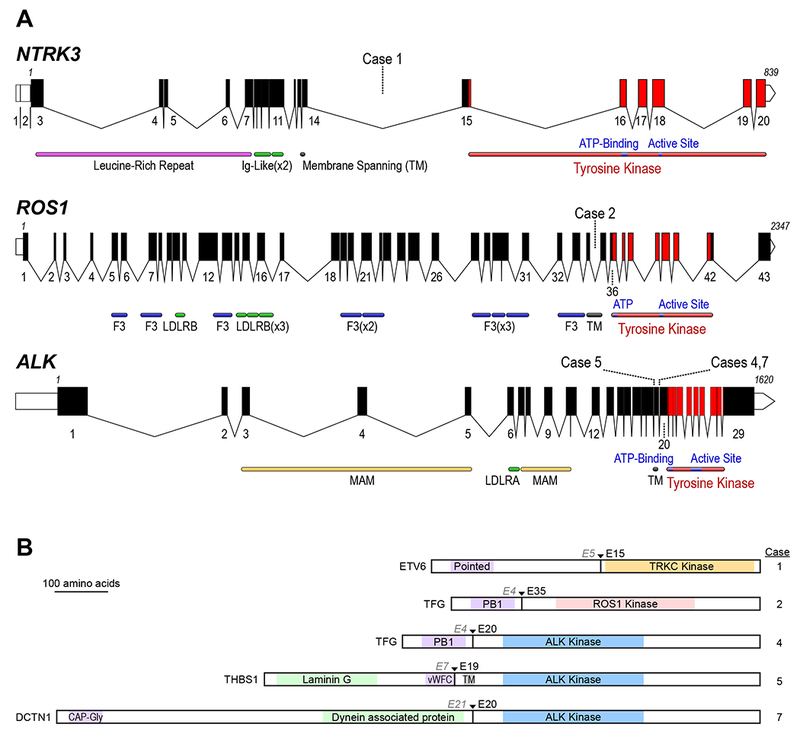
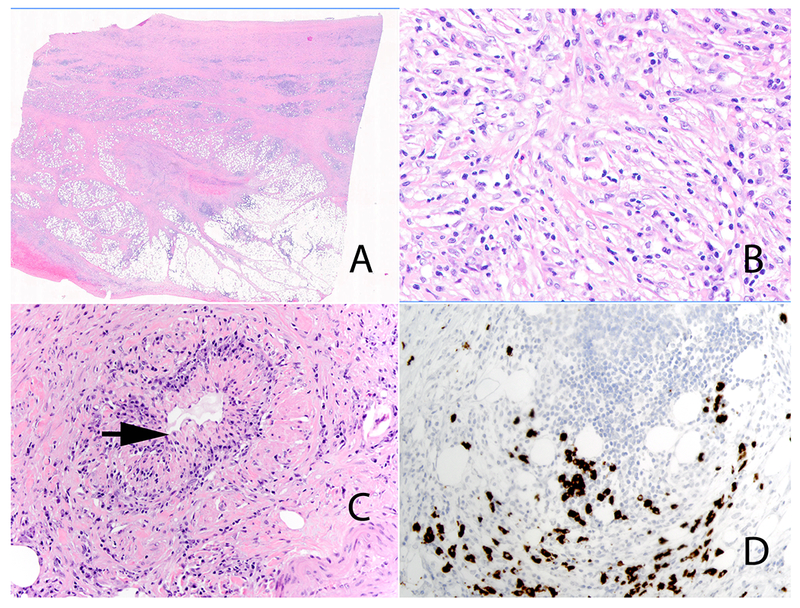
Inflammatory myofibroblastic tumor (IMT), a locally aggressive neoplasm capable of metastasis, may show an immunoglobulin (Ig)G4-rich lymphoplasmacytic infiltrate. Prior reports suggest that storiform-fibrosis and obliterative phlebitis aid in the distinction of IMT from IgG4-related diseases. Herein, we highlight the morphologic overlap between the 2 diseases, and emphasize the importance of a multiplex fusion assay in the distinction of IgG4-related disease (IgG4-RD) from IMT. We identified 7 IMTs with morphologic and immunohistochemical features of IgG4-RD; 3 patients were originally diagnosed with IgG4-RD. Demographic, clinical and morphologic data was recorded. We also reevaluated 56 patients with IgG4-RD. We performed immunohistochemistry for IgG4, IgG, ALK, and ROS1. In situ hybridization for IgG4 and IgG was performed in selected cases. A multiplex next-generation sequencing-based RNA assay for gene fusions was performed to detect all known IMT-related gene fusions. All 7 IMTs showed a dense lymphoplasmacytic infiltrate and storiform-type fibrosis, with obliterative phlebitis noted in 3 cases. The neoplastic stromal cells constituted <5% of overall cellularity and stromal atypia was either absent or focal and mild. Elevated numbers of IgG4 positive cells and increased IgG4 to IgG ratio was identified in all cases. Four cases showed ALK related abnormalities: 3 fusions and one alternative transcription initiation; while 2 patients showed ROS1 and NTRK3 fusions. One tumor was negative for known IMT-related gene fusions. All 56 IgG4-RD cases were negative for ALK and ROS1 on immunohistochemistry; 6 cases were negative on the fusion assay. Highly inflamed IMTs are indistinguishable from IgG4-RD both histologically and on immunohistochemistry for IgG4. We advocate scrutinizing patients with presumptive single organ IgG4-RD for IMT and the diagnostic algorithm should include ALK and ROS1 immunohistochemistry and, in selected cases, a next-generation sequencing-based fusion assay that covers known IMT-associated gene fusions.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
