

Microbleeds and Cerebral Amyloid Angiopathy in the Brains of People with Down Syndrome with Alzheimer's Disease
- PMID: 30452414
- PMCID: PMC6424116
- DOI: 10.3233/JAD-180589
Microbleeds and Cerebral Amyloid Angiopathy in the Brains of People with Down Syndrome with Alzheimer's Disease
Abstract
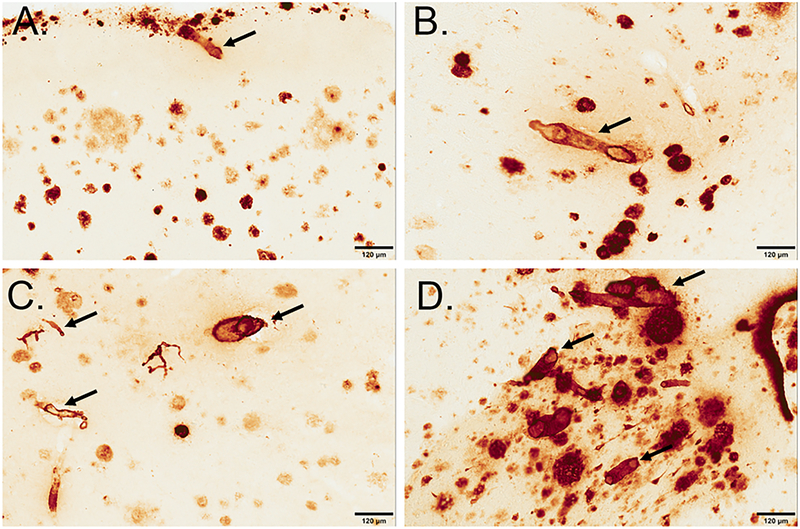
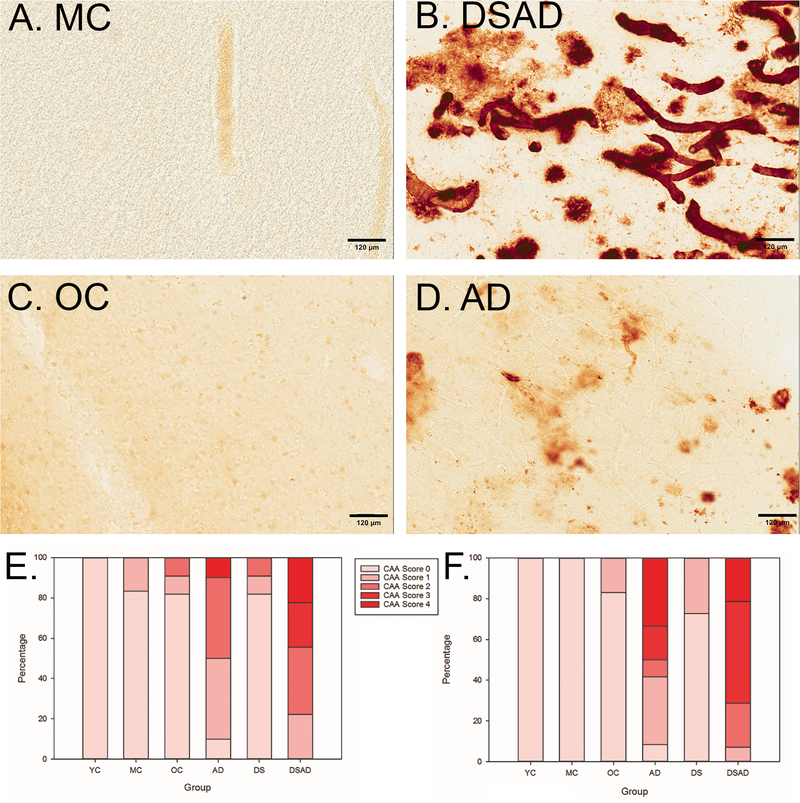
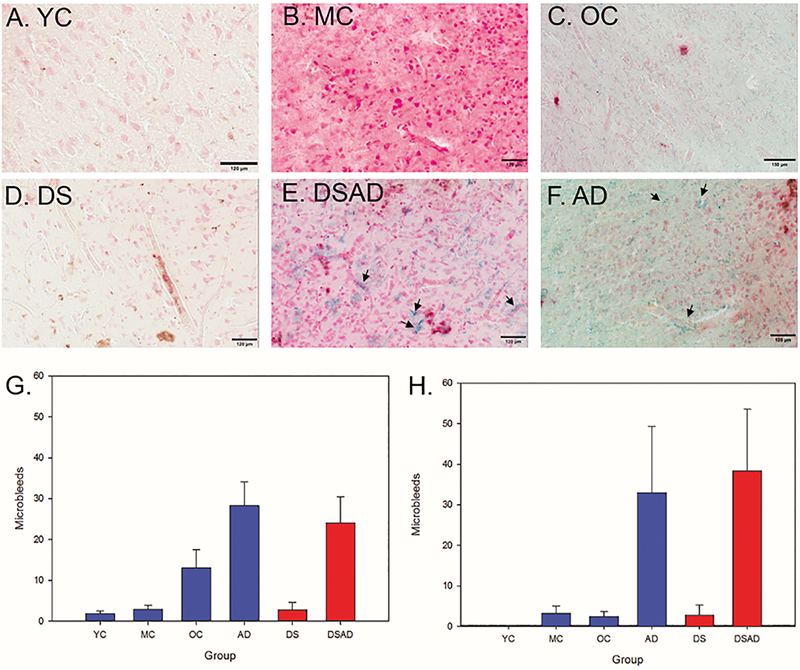
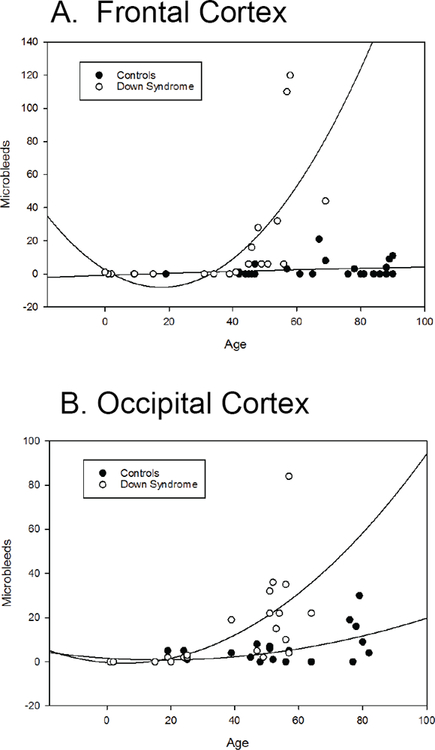
Cerebrovascular pathology is a significant mediator in Alzheimer's disease (AD) in the general population. In people with Down syndrome (DS), the contribution of vascular pathology to dementia may play a similar role in age of onset and/or the rate of progression of AD. In the current study, we explored the extent of microbleeds (MBs) and the link between cerebral amyloid angiopathy (CAA) and MBs in the frontal cortex (FCTX) and occipital cortex (OCTX) in an autopsy series from individuals with DS (<40 years), DS with AD pathology (DSAD), sporadic AD, and control cases (2-83 years). Sections were immunostained against Aβ1 - 40 and an adjacent section stained using Prussian blue for MBs. MBs were both counted and averaged in each case and CAA was scored based on previously published methods. MBs were more frequent in DS cases relative to controls but present to a similar extent as sporadic AD. This aligned with CAA scores, with more extensive CAA in DS relative to controls in both brain regions. CAA was also more frequent in DSAD cases relative to sporadic AD. We found CAA to be associated with MBs and that MBs increased with age in DS after 30 years of age in the OCTX and after 40 years of age in the FCTX. MB and CAA appear to be a significant contributors to the development of dementia in people with DS and are important targets for future clinical trials.
Keywords: Cerebral amyloid angiopathy; Prussian blue; microhemorrhages; trisomy 21.
Figures
Similar articles
-
Cerebral amyloid angiopathy in Down syndrome and sporadic and autosomal-dominant Alzheimer's disease.Alzheimers Dement. 2017 Nov;13(11):1251-1260. doi: 10.1016/j.jalz.2017.03.007. Epub 2017 Apr 29. Alzheimers Dement. 2017. PMID: 28463681 Free PMC article.
-
Patterns and severity of vascular amyloid in Alzheimer's disease associated with duplications and missense mutations in APP gene, Down syndrome and sporadic Alzheimer's disease.Acta Neuropathol. 2018 Oct;136(4):569-587. doi: 10.1007/s00401-018-1866-3. Epub 2018 May 16. Acta Neuropathol. 2018. PMID: 29770843 Free PMC article.
-
Cerebrovascular pathology in Down syndrome and Alzheimer disease.Acta Neuropathol Commun. 2017 Dec 1;5(1):93. doi: 10.1186/s40478-017-0499-4. Acta Neuropathol Commun. 2017. PMID: 29195510 Free PMC article.
-
Cerebrovascular contributions to aging and Alzheimer's disease in Down syndrome.Biochim Biophys Acta. 2016 May;1862(5):909-14. doi: 10.1016/j.bbadis.2015.11.007. Epub 2015 Nov 26. Biochim Biophys Acta. 2016. PMID: 26593849 Free PMC article. Review.
-
Down syndrome, Alzheimer disease, and cerebral amyloid angiopathy: The complex triangle of brain amyloidosis.Dev Neurobiol. 2019 Jul;79(7):716-737. doi: 10.1002/dneu.22709. Epub 2019 Aug 5. Dev Neurobiol. 2019. PMID: 31278851 Review.
Cited by
-
Alzheimer-Related Cerebrovascular Disease in Down Syndrome.Ann Neurol. 2020 Dec;88(6):1165-1177. doi: 10.1002/ana.25905. Epub 2020 Oct 9. Ann Neurol. 2020. PMID: 32944999 Free PMC article.
-
Cholinergic System Structure and Function Changes in Individuals with Down Syndrome During the Development of Alzheimer's Disease.Curr Top Behav Neurosci. 2025;69:49-78. doi: 10.1007/7854_2024_523. Curr Top Behav Neurosci. 2025. PMID: 39485646 Review.
-
Neuropathology of trisomy 21 mosaicism in a case with early-onset dementia.Alzheimers Dement. 2025 Jan;21(1):e14394. doi: 10.1002/alz.14394. Epub 2024 Dec 10. Alzheimers Dement. 2025. PMID: 39655579 Free PMC article.
-
A pathway linking pulse pressure to dementia in adults with Down syndrome.Brain Commun. 2024 May 9;6(3):fcae157. doi: 10.1093/braincomms/fcae157. eCollection 2024. Brain Commun. 2024. PMID: 38764776 Free PMC article.
-
Alzheimer's Disease Research Center Down Syndrome Cores: Experience from two sites.Alzheimers Dement. 2025 Aug;21(8):e70612. doi: 10.1002/alz.70612. Alzheimers Dement. 2025. PMID: 40847661 Free PMC article. Review.
References
-
- Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, Anderson P, Mason CA, Collins JS, Kirby RS, Correa A (2010) Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Res A Clin Mol Teratol 88, 1008–1016. - PubMed
-
- Dierssen M (2012) Down syndrome: the brain in trisomic mode. Nat Rev Neurosci 13, 844–858. - PubMed
-
- Glasson EJ, Sullivan SG, Hussain R, Petterson BA, Montgomery PD, Bittles AH (2002) The changing survival profile of people with Down’s syndrome: implications for genetic counselling. Clin Genet 62, 390–393. - PubMed
-
- Bittles AH, Bower C, Hussain R, Glasson EJ (2007) The four ages of Down syndrome. Eur J Public Health 17, 221–225. - PubMed
-
- Hartley D, Blumenthal T, Carrillo M, DiPaolo G, Esralew L, Gardiner K, Granholm AC, Iqbal K, Krams M, Lemere C, Lott I, Mobley W, Ness S, Nixon R, Potter H, Reeves R, Sabbagh M, Silverman W, Tycko B, Whitten M, Wisniewski T (2015) Down syndrome and Alzheimer’s disease: Common pathways, common goals. Alzheimers Dement 11, 700–709. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
