

A decade of catheter ablation of cardiac arrhythmias in Sweden: ablation practices and outcomes
- PMID: 30452631
- PMCID: PMC6403459
- DOI: 10.1093/eurheartj/ehy709
A decade of catheter ablation of cardiac arrhythmias in Sweden: ablation practices and outcomes
Abstract
Aims: Catheter ablation is considered the treatment of choice for many tachyarrhythmias, but convincing 'real-world' data on efficacy and safety are lacking. Using Swedish national registry data, the ablation spectrum, procedural characteristics, as well as ablation efficacy and reported adverse events are reported.
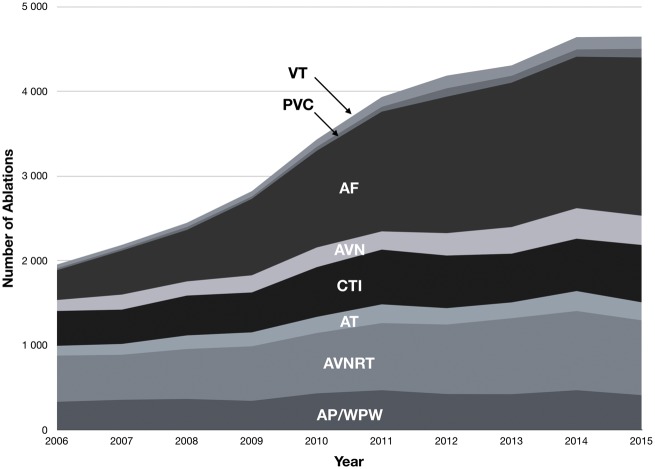
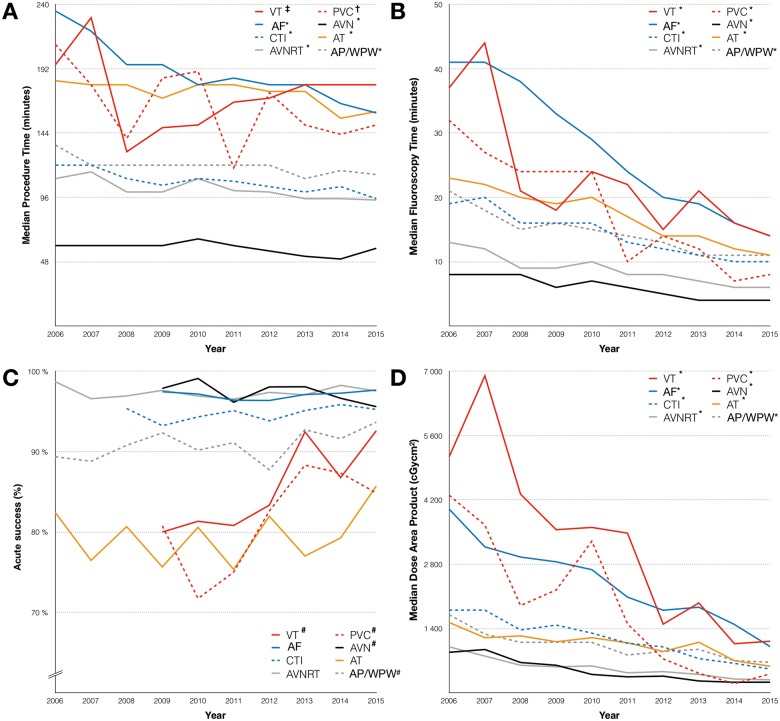
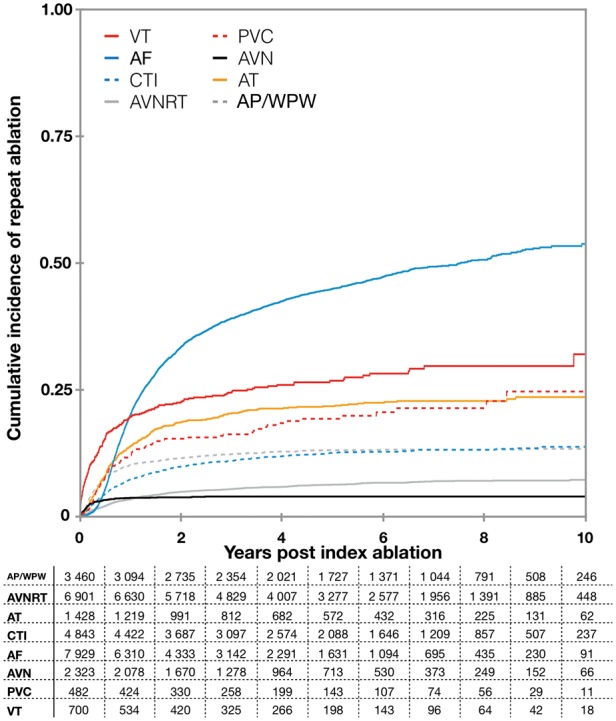
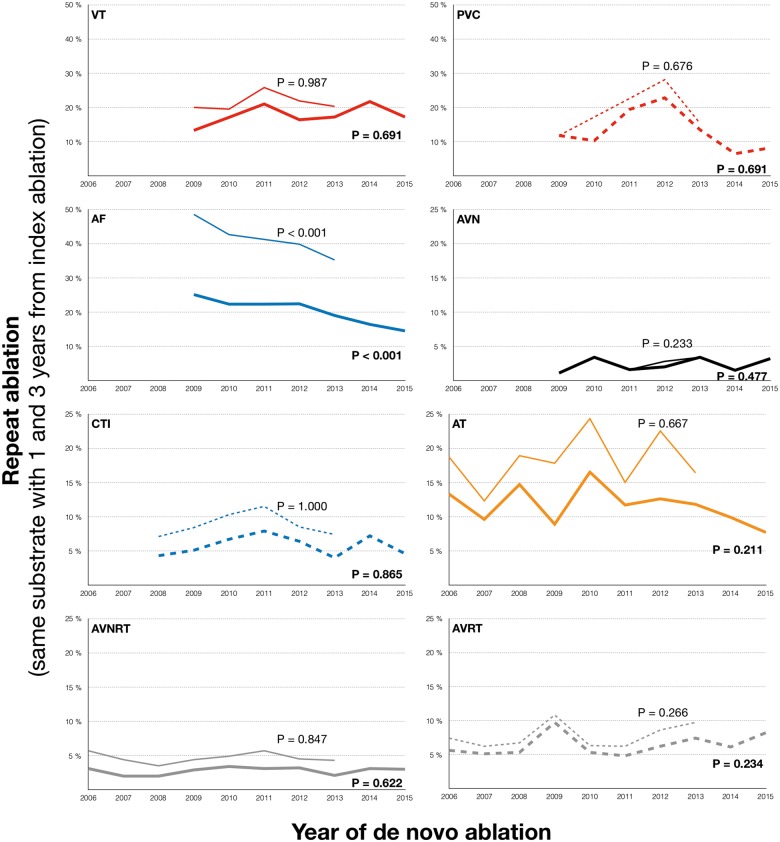
Methods and results: Consecutive patients (≥18 years of age) undergoing catheter ablation in Sweden between 01 January 2006 and 31 December 2015 were included in the study. Follow-up (repeat ablation and vital status) was collected through 31 December 2016. A total of 26 642 patients (57 ± 15 years, 62% men), undergoing a total of 34 428 ablation procedures were included in the study. In total, 4034 accessory pathway/Wolff-Parkinson-White syndrome (12%), 7358 AV-nodal re-entrant tachycardia (21%), 1813 atrial tachycardia (5.2%), 5481 typical atrial flutter (16%), 11 916 atrial fibrillation (AF, 35%), 2415 AV-nodal (7.0%), 581 premature ventricular contraction (PVC, 1.7%), and 964 ventricular tachycardia (VT) ablations (2.8%) were performed. Median follow-up time was 4.7 years (interquartile range 2.7-7.0). The spectrum of treated arrhythmias changed over time, with a gradual increase in AF, VT, and PVC ablation (P < 0.001). Decreasing procedural times and utilization of fluoroscopy with time, were seen for all arrhythmia types. The rates of repeat ablation differed between ablation types, with the highest repeat ablation seen in AF (41% within 3 years). The rate of reported adverse events was low (n = 595, 1.7%). Death in the immediate period following ablation was rare (n = 116, 0.34%).
Conclusion: Catheter ablations have shifted towards more complex procedures over the past decade. Fluoroscopy time has markedly decreased and the efficacy of catheter ablation seems to improve for AF.
Keywords: Adverse events; Catheter ablation; Outcome.
© The Author(s) 2018. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Catheter ablation: an ongoing revolution.J Thorac Dis. 2019 Mar;11(Suppl 3):S212-S215. doi: 10.21037/jtd.2019.02.20. J Thorac Dis. 2019. PMID: 30997179 Free PMC article. No abstract available.
References
-
- Gallagher JJ, Svenson RH, Kasell JH, German LD, Bardy GH, Broughton A, Critelli G.. Catheter technique for closed-chest ablation of the atrioventricular conduction system. N Engl J Med 1982;306:194–200. - PubMed
-
- Borggrefe M, Budde T, Podczeck A, Breithardt G.. High frequency alternating current ablation of an accessory pathway in humans. J Am Coll Cardiol 1987;10:576–582. - PubMed
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J.. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659–666. - PubMed
-
- Stevenson WG, Delacretaz E, Friedman PL, Ellison KE.. Identification and ablation of macroreentrant ventricular tachycardia with the CARTO electroanatomical mapping system. Pacing Clin Electrophysiol 1998;21:1448–1456. - PubMed
-
- Novak PG, Macle L, Thibault B, Guerra PG.. Enhanced left atrial mapping using digitally synchronized NavX three-dimensional nonfluoroscopic mapping and high-resolution computed tomographic imaging for catheter ablation of atrial fibrillation. Heart Rhythm 2004;1:521–522. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
